


Bubble Study
The reason to perform a bubble study is to confirm the presence of shunting of blood from venous to arterial flow such as a Reverse VSD or a Reverse PDA.

Gallbladder Motility Study
NPO overnight. Time 0 min: Measure GB in long axis and short axis from subxiphoid approach and right intercostal approach. The proper position is maximum

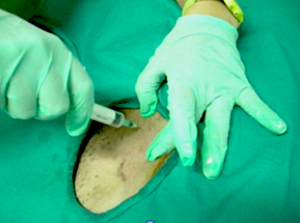
Lindquist Compression Technique For Thoracic FNA
This technique often makes inaccessible thoracic lesions accessible.
Traumatic Catheterization Procedure
Sedation Use largest open-end rigid polypropylene urinary catheter cut diagonally to create a sharp edge like a needle bevel. Lube heavily and pass catheter retrograde
UGELAB for Transitional Cell Carcinoma in the Dog
Dr. Dean Cerf, Ridgewood Veterinary Hospital NJ and Dr. Eric Lindquist, SonoPath.com For More Information Contact Dr. Dean Cerf at Ridgewood Veterinary Hospital, Ridgewood, NJ,

Ultrasound-Guided Lymph Node Culture
This type of lymph node sampling is helpful in determining infected lymph nodes vs. lymphoma. Supplies: 6 cc Luer lock syringe 1cc of saline 2
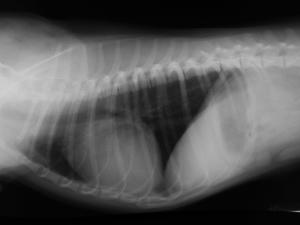
Ultrasound-Guided Pericardiocentesis
History Pericardial effusions typically cause some level of cardiomegaly on radiographs but note poor vascular volume in the pulmonary artery and vein. Muffled heart sounds

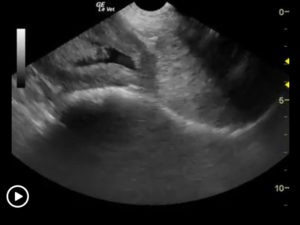
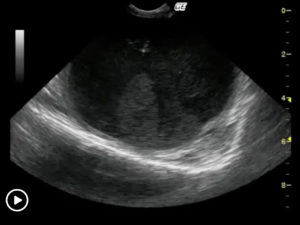
Ultrasound-Guided Sampling Procedures
Description Ultrasound-guided needle sampling is frequently used in the diagnostic evaluation of patients. Fine needle aspiration has the advantage of requiring minimal or no sedation