We would like to thank Dr. McAleer for the referral and dedicated care provided to our recent canine patient. We’re grateful to Brodheadsville Veterinary Clinic for their continued support and trusted collaboration. Special thanks to Becca Hamilton, SDEP® Certified Clinical Sonographer with SonoPath’s NJ Mobile team, for her thorough and high-quality imaging, and to Eric Lindquist, DMV, DABVP, Cert. IVUSS, for his expert analysis, which offered valuable guidance for case management. This case serves as a great example of how collaborative efforts lead to the highest standard of care.

Presenting Clinical Signs:
The patient presented with persistently elevated liver enzymes and bilateral abdominal cryptorchidism.
Abnormal Diagnostic Findings:
Urine Specific Gravity (USG): 1.047 – Concentrated urine
Complete Blood Count (CBC): Lymphocytosis (Lymphocytes: 5,336/µL – High)
Serum Chemistry Panel:
- Blood Urea Nitrogen (BUN): 5 mg/dL – Low
- Creatinine: 0.4 mg/dL – Low
- Alanine Aminotransferase (ALT): 403 U/L – High
- Alkaline Phosphatase (ALP): 175 U/L – High
Urinalysis:
Crystalluria noted with both calcium oxalate and ammonium phosphate crystals



ULTRASONOGRAPHIC EXAMINATION OF THE ABDOMEN
Urinary System:
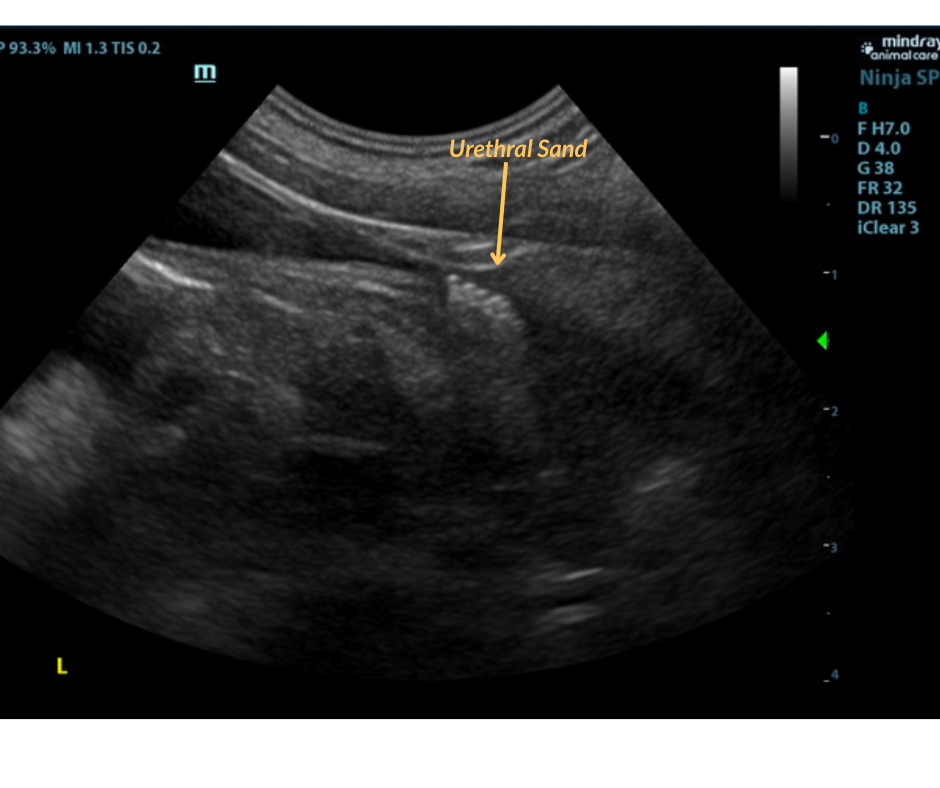
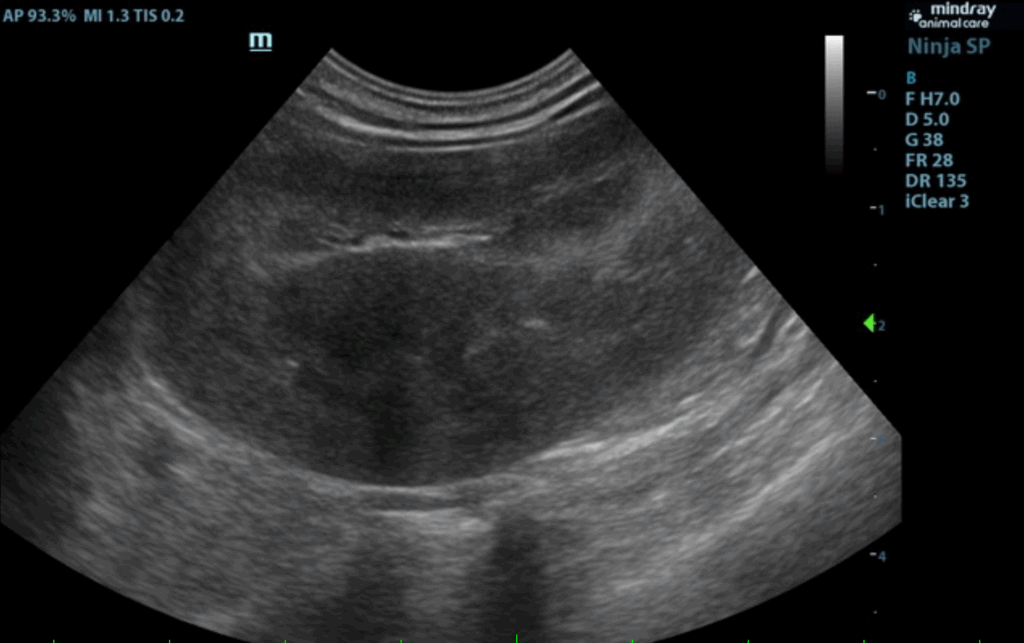
The urinary bladder and visible pelvic urethra were unremarkable for the level of repletion presented.The urine, however, did present some mildly echogenic debris consistent with mucous, exfoliated cells from renal or bladder origin, and/or blood clots as these echogenic changes can all present similarly. A minor amount of urethral sand was noted just prior to the prostate. The prostate measured 1.5 cm. The kidneys were both swollen with hypervascularity. This is likely owing to abnormal ammonia metabolism. The right kidney measured 5.33 cm. The left kidney measured 5.16 cm. Both testicles were retained and were inguinal and extra-abdominal.
Adrenal Glands:
Both adrenal glands were visualized and recognized as having normal shape, size, position and echogenicity for this breed. The phrenic vasculature, glandular echogenicity and detail were unremarkable. Capsule, cortex, and medullary definition were normal for this age patient. The left adrenal gland measured 1.96 x 0.27 cm at the cranial pole and 0.27 cm at the caudal pole. The right adrenal gland measured 1.4 x 0.45 cm at the cranial pole and 0.3 cm at the caudal pole.
Spleen:
The spleen in this patient was mildly enlarged with uniform parenchyma and was folded upon itself caudally. This is a positional variant and is not pathological. There was no evidence of significant disease.
Liver:
The liver was mildly subnormal in size. The hepatic parenchyma was uniform, yet hypovascular owing to the extrahepatic shunting. The extrahepatic shunt decoursed ventral caudally and then dorsally. It appeared to bypass the vena cava and aorta. It likely entered into the azygos, however, the termination
could not be found given the lack of acoustic window. The hepatic width was approximately 2.0 cm in short axis. The portal vein was subnormal in size and measured 0.34 cm after the gastroduodenal vein junction. An extrahepatic vessel was present just caudal to the pylorus and measured 1.05 cm. This is
consistent with gastric shunt. The aorta and vena cava both measured approximately 0.65 cm. The gallbladder and common bile were unremarkable.
Gastrointestinal:
The gastric wall was mildly thickened likely owing to gastritis and abnormal ammonia metabolism. The small intestines and colon were unremarkable.
Pancreas:
The base and limbs of the pancreas were observed to be largely isoechoic to surrounding omental fat. Pancreatic duct and capsular contour were acceptably normal and parenchyma respected normal curvilinear patterns. No overt evidence of active inflammatory or neoplastic disease was noted.
ULTRASONOGRAPHIC FINDINGS
- Extrahepatic portosystemic shunt. Gastroazygos or gastrophrenic shunt is suspected.
- Concurrent gastritis pattern.
- Inguinal, extra-abdominal testicles, surgically accessible without entering the abdominal cavity.
- Bladder sand and debris.
- Swollen, hypervascular kidneys.
INTERPRETATION OF THE FINDINGS & FURTHER RECOMMENDATIONS:
CT evaluation for surgical planning is recommended. This is a particularly large shunt resulting in large shunt fraction. Therefore, there is a risk of portal hypertension secondary to surgical attenuation. The patient should be imaged 24-48 hours post surgery to ensure that portal hypertension is not developing with pancreatic edema. Liver biopsy is warranted at the time of the sonogram.
————————————————————————————————————-
A computed tomography (CT) scan was subsequently performed, which confirmed the presence and specific location of the shunt, providing valuable information for guiding the next steps in the pet’s surgical plan.
INTERPRETATION OF THE CT FINDINGS:
- Single extrahepatic portosystemic shunt, connecting from the right gastric vein via the left gastric vein, which receives the splenic vein, to the caudal vena cava.
- An additional abnormal connection of the left pancreatic vein to the portal vein appears to be present in the region of the expected entrance location of the splenic vein.
- Associated mild microhepatia.
- Associated cystourolithiasis

The Gastroduodenal vein (GDV) and splenic vein normally empty into the portal vein (PV) separately like the above image.
In this patient, the gastroduodenal vein receives the splenic vein, is enlarged and empties abnormally into the caudal vena cava.


Discussion:
A portosystemic shunt is an abnormal vessel that redirects blood from the portal circulation into the systemic circulation. They are either congenital or acquired, single or multiple, extrahepatic or intrahepatic. Single congenital extrahepatic shunts are the most common and are usually seen in toy and small breed dogs like the Shih Tzu. Extrahepatic shunts (EHPSS) connect the portal vein or one of its tributaries to the caudal vena cava or azygos vein. The most common types are splenoazygous, splenocaval, and splenophrenic. Less commonly seen shunts are right gastrocaval, double right gastrocaval, and double right gastroazygos.
In normal animals blood from the intestines, pancreas, spleen, and stomach enters the liver through the portal system. This blood contains hormones from the pituitary gland, toxins from the intestines and bacterial products. When an EHPSS exists portal blood bypasses the liver and enters directly into systemic circulation. The liver fails to develop properly, there is decreased protein production, and abnormal fat and protein metabolism. Toxins and byproducts that are usually metabolized or eliminated by the liver then build up in the body. When these reach a certain level hepatic encephalopathy, gastrointestinal signs, poor growth, coagulopathies, and lower urinary tract signs will develop.
Ultrasound can identify a small liver, abnormal vessels, altered portal vein/vena cava ratio, altered portal vein/aorta ratio, renomegaly, and urolithiasis. Identification of a EHPSS with an experienced operator has an 80% sensitivity and 90% specificity. CT scan is used for cases that are unable to be identified using ultrasound and to correctly identify the origin and end point of the shunt for surgical planning.
Surgery and Patient Outcome:
The patient was referred to a specialist for surgical correction of the shunt, neuter, and cystotomy. The surgery was successful, and the patient has recovered remarkably well, resuming a happy and normal life. Post-operatively, a liver biopsy and cystolith were submitted for histopathology and stone analysis, providing additional insights into the underlying pathology. The patient is now thriving, free from the complications of the shunt, and continues to enjoy a full, healthy life.

Excisional Liver Biopsy


Liver Biopsy:
Liver: Lobular hypoplasia, diffuse, chronic, moderate, with hepatocellular atrophy, arteriolar reduplication, and mild biliary hyperplasia. The vascular changes in this liver represent a stereotypic response to insufficient portal blood supply resulting from either a congenital shunt, portal vein hypoplasia (microvascular dysplasia), or acquired portal hypertension due to cirrhosis or extrahepatic causes.
Stone Analysis
100% Ammonium acid urate.
References
1. Devriendt N, Serrano G, Stock E, et al. Diagnostic value of liver function tests and ultrasonography in dogs with suspected congenital portosystemic shunts. Veterinary Record 2022;190:e1381.
2. Adam FH, German AJ, McConnell JF, et al. Clinical and clinicopathologic abnormalities in young dogs with acquired and congenital portosystemic shunts: 93 cases (2003–2008). 2012. Available at: https://avmajournals.avma.org/view/journals/javma/241/6/javma.241.6.760.xml. Accessed July 28, 2025.
3. White RN, Parry AT. Morphology of splenocaval congenital portosystemic shunts in dogs and cats. Journal of Small Animal Practice 2016;57:28–32.
4. D’Anjou M-A, Penninck D, Cornejo L, et al. Ultrasonographic Diagnosis of Portosystemic Shunting in Dogs and Cats. Veterinary Radiology & Ultrasound 2004;45:424–437.
Looking to enhance the range of your ultrasound diagnostic efficiency?
