
History:
The patient presented with lethargy, marked cachexia, and weak peripheral pulses. Thoracic radiographs were suggestive for an enlarged cardiac silhouette, while abdominal radiographs were suspicious for diffuse hepatosplenomegaly. The patient had recently completed a three-week course of doxycycline for a fever of unknown origin (FUO), with a negative tick-borne disease PCR panel.
Thank you to Dr. Hartelius for the referral and excellent case management of our recent canine patient. A special shoutout to Rondout Valley Veterinary Associates for their continued trust and collaboration. We’re also grateful to Meghan Morse, A.A.S Veterinary Technology , LVT, CVT: NJ Mobile, SDEP® Clinical Sonographer for her detailed imaging, and to Eric Lindquist, DMV, DABVP, Cert. IVUSS, Founder & CEO of SonoPath for his exceptional interpretation, which provided invaluable insights for the case.

Current medications include prednisolone at 20 mg/day and gabapentin at 600 mg/day, prescribed for cervical pain that began approximately one month prior. Recent diagnostic results revealed several abnormalities: albumin 2.7 g/dL, ALKP 184 U/L, ALT 220 U/L, BUN 33 mg/dL, creatinine 2.1 mg/dL, WBC 15,000/µL with a mature neutrophilia, hematocrit 53.2%, and platelet count 120,000/µL (refer to detailed bloodwork values below).




Performing both an abdominal ultrasound and an echocardiogram is essential for comprehensive diagnostic evaluation in many veterinary patients, particularly when systemic or multi-organ disease is suspected. Abdominal ultrasonography enables detailed visualization of visceral organs such as the liver, spleen, kidneys, gastrointestinal tract, and reproductive organs, aiding in the diagnosis of neoplasia, inflammation, fluid accumulation, organ dysfunction or other. Meanwhile, echocardiography provides real-time assessment of cardiac structure and function, allowing for the detection of conditions such as valvular disease, cardiomyopathies, pericardial effusion, and congenital heart defects. In many cases, concurrent disease in the heart and abdomen—such as cardiac-related ascites, neoplastic syndromes, or systemic infections—necessitates evaluation of both cavities to guide accurate diagnosis and appropriate treatment. Utilizing both modalities enhances diagnostic accuracy, supports risk assessment before anesthesia or surgery, and improves clinical decision-making in complex cases, ultimately contributing to better outcomes in veterinary patients.


ULTRASONOGRAPHIC EXAMINATION OF THE ABDOMEN:
Urinary System
The urinary bladder, trigone, and pelvic urethra presented normal thicknesses and normal tone. The
ureters were not visible which is normal. No uroliths or sediment were visualized and anechoic urine
was present. No evidence of inflammatory or neoplastic changes was noted. Ureteral papillae were
normal.
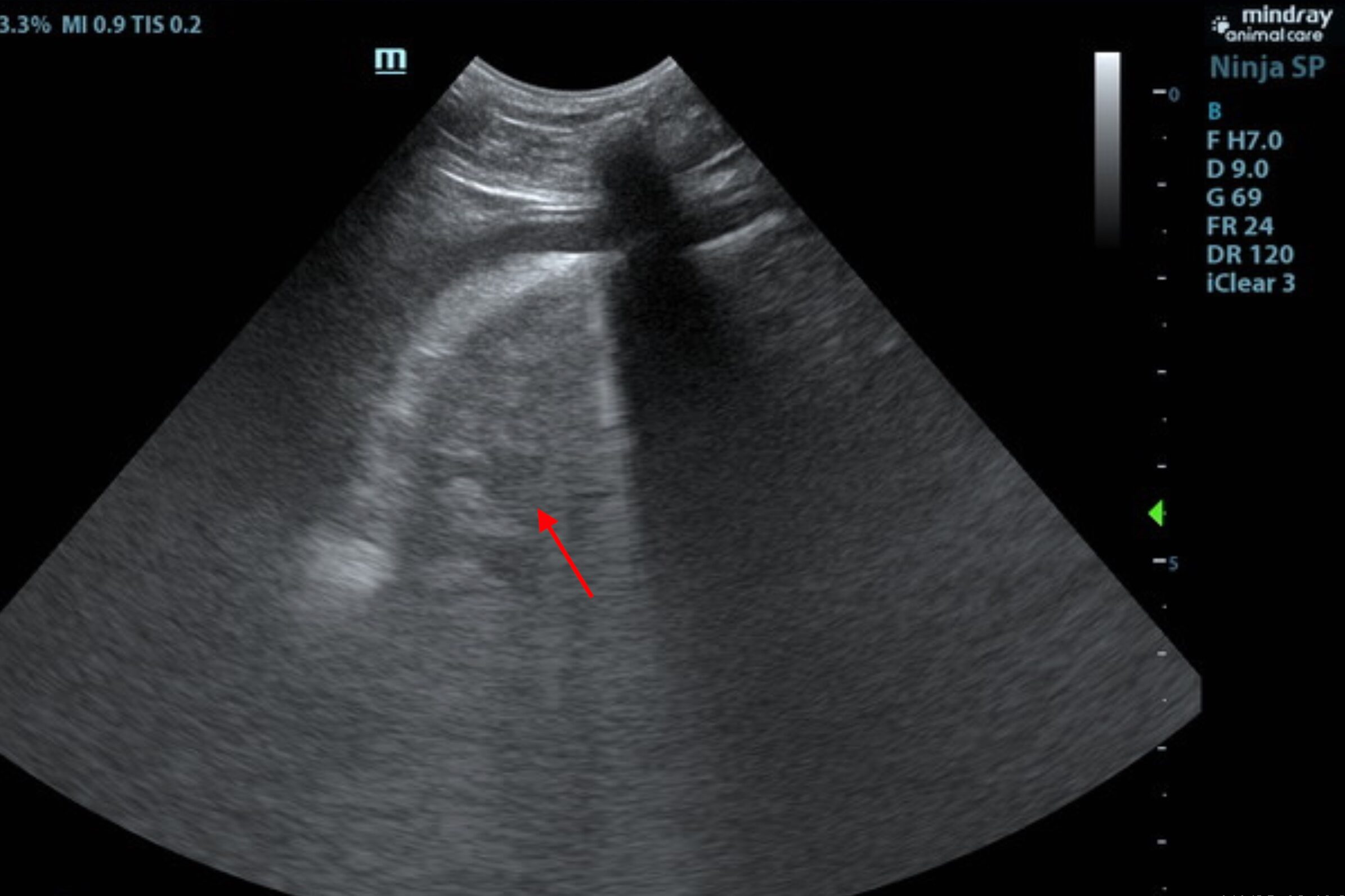
The kidneys revealed largely normal size and structure, corticomedullary definition and ratio (cortex
1/3 of medulla) were essentially maintained with some age-related loss of curvilinear patterns regarding
the capsule and C/M junction. The cortices presented largely uniform texture with some increased
echogenicity expected for his age patient. Medullary structure differed distinctly from that of the cortex
and no evidence of pelvic dilation was present. A cortical infarct was noted in the dorsal cortex of the
right kidney. The right kidney measured 7.2 cm. The left kidney measured 6.99 cm.
Adrenal Glands
Both adrenal glands were visualized and recognized as having normal shape, size, position and
echogenicity for this breed. The phrenic vasculature, glandular echogenicity and detail were
unremarkable. Capsule, cortex, and medullary definition were normal for this age patient. The left
adrenal gland measured 2.15 x 0.45 cm at the caudal pole and 0.6 cm at the cranial pole. The right
adrenal gland measured 2.0 x 0.78 cm at the caudal pole and 0.63 cm at the cranial pole.
Spleen
The spleen presented a smooth homogeneous parenchyma hyperechoic to liver and renal cortical
parenchyma. The capsule was smooth without noticeable expansion or deviation from within the spleen
or adjacent pathology. The splenic vasculature demonstrated normal volume without signs of
congestion or thrombosis. No sonographic evidence of acute or chronic inflammatory, neoplastic, or
infarctual changes was noted.
Liver
The liver images from right and left intercostal as well as subcostal views revealed subjectively normal
liver size, contour, and structure. Some age-related parenchymal remodeling was noted but likely not clinically significant at this time. Vascular and biliary tracts were of normal volume and no evidence of
congestion was noted. The gallbladder presented some dependent debris with essentially normal
contour. The cystic and common bile ducts were normal. No overt evidence of active inflammatory,
infiltrative or regenerative pathology was noted but should be paired with current or past LE elevations
regarding any clinical significance to this presentation. The hepatic lymph nodes were unremarkable.
Gastrointestinal
Examination of the gastrointestinal tract revealed a stomach and intestine free of stasis, of normal wall
thickness, acceptable curvilinear mural detail, and peristaltic activity. Small and large intestine
demonstrated normal luminal chyme and stool consistency respectively. No obstructive or overt
infiltrative disease was noted. No associated abnormal lymphatic activity was noted.
Pancreas
The right limb of the pancreas was heterogenous with mixed, hypoechoic parenchymal changes and
irregular contour.
Free Abdomen
Iliac trifurcation was unremarkable. There was no evidence of thrombosis.
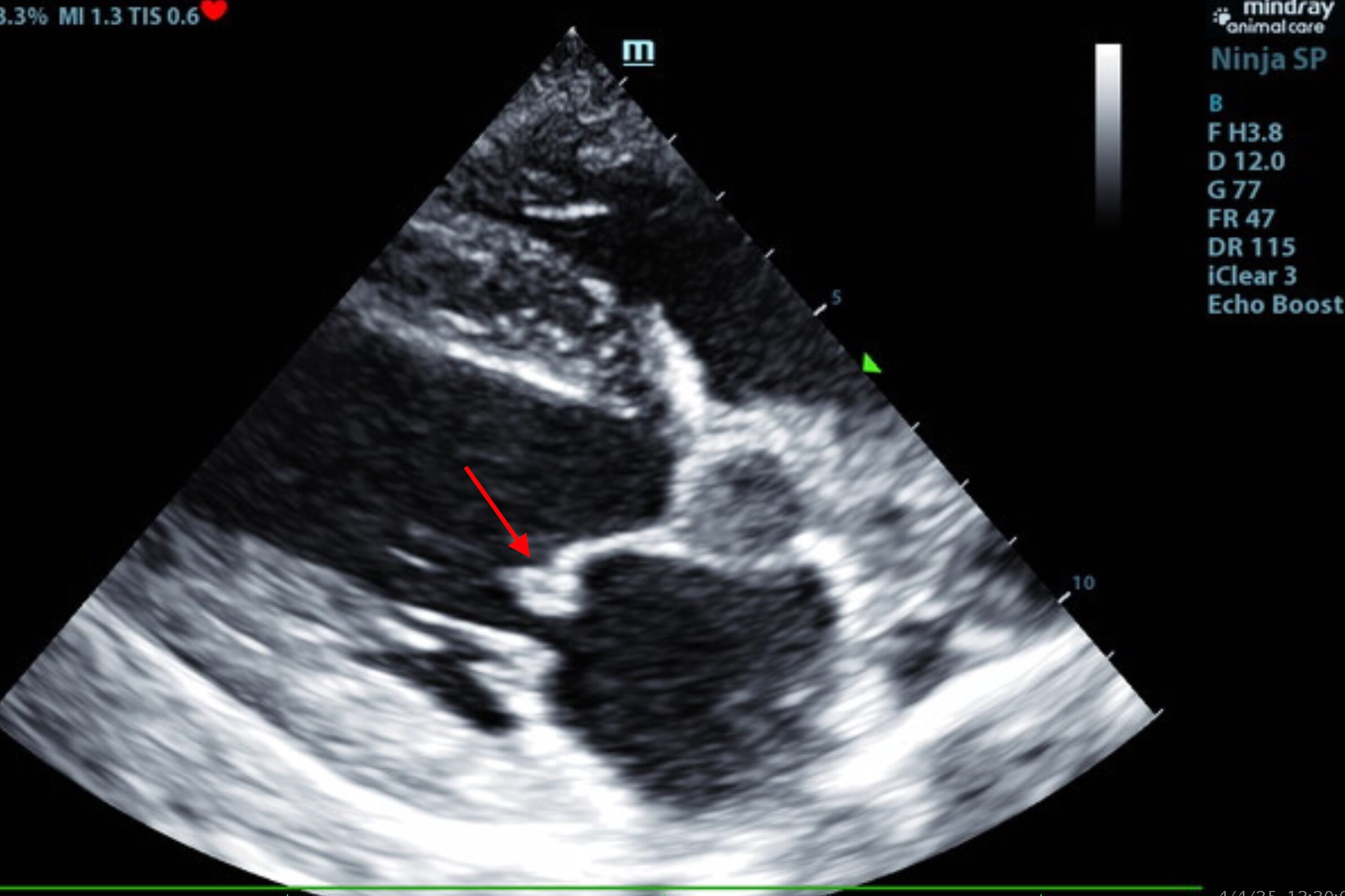
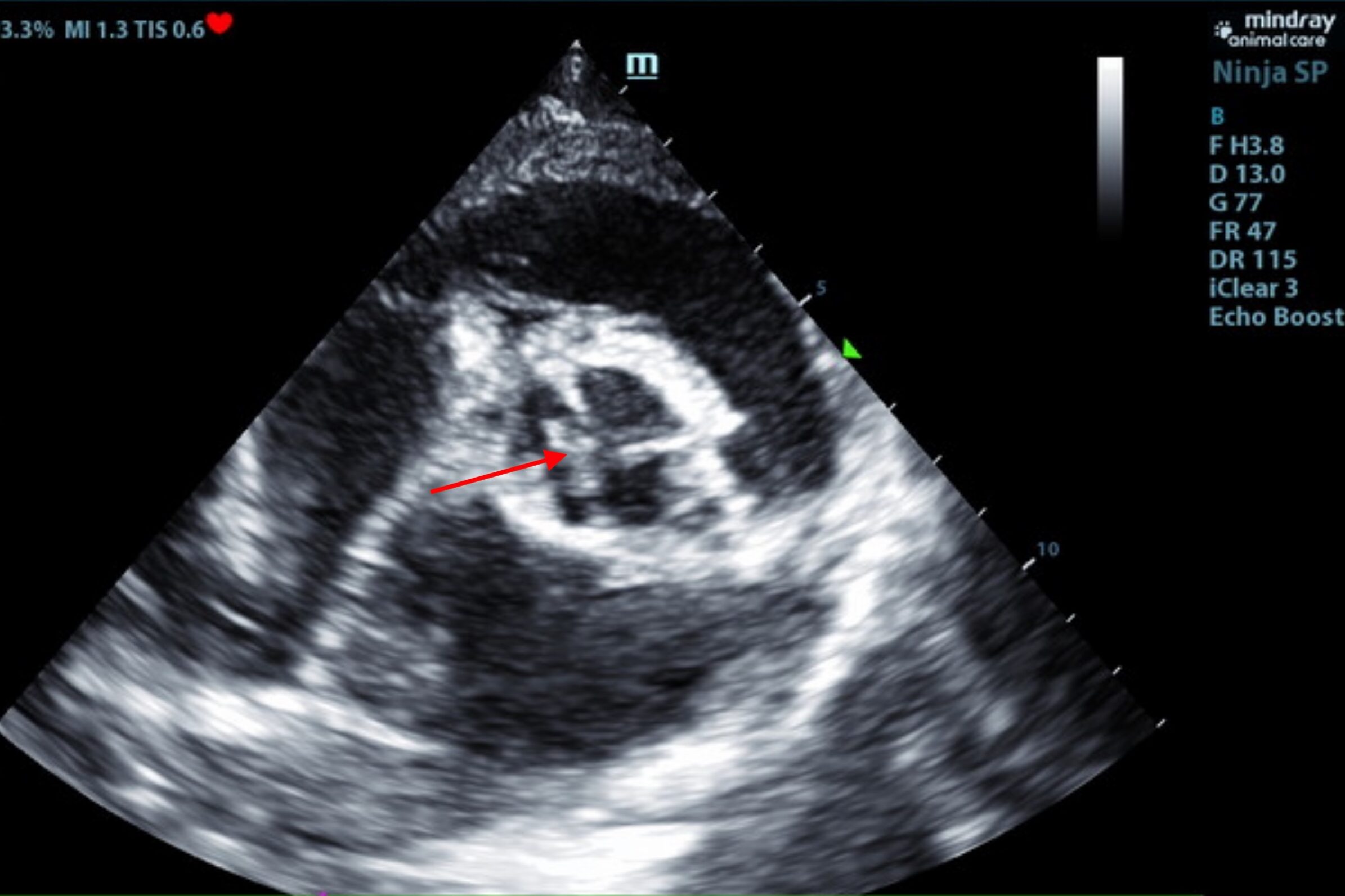
ULTRASONOGRAPHIC EXAMINATION OF THE HEART
The echocardiogram in this patient demonstrated normal left atrial size based on 3 separate methods of
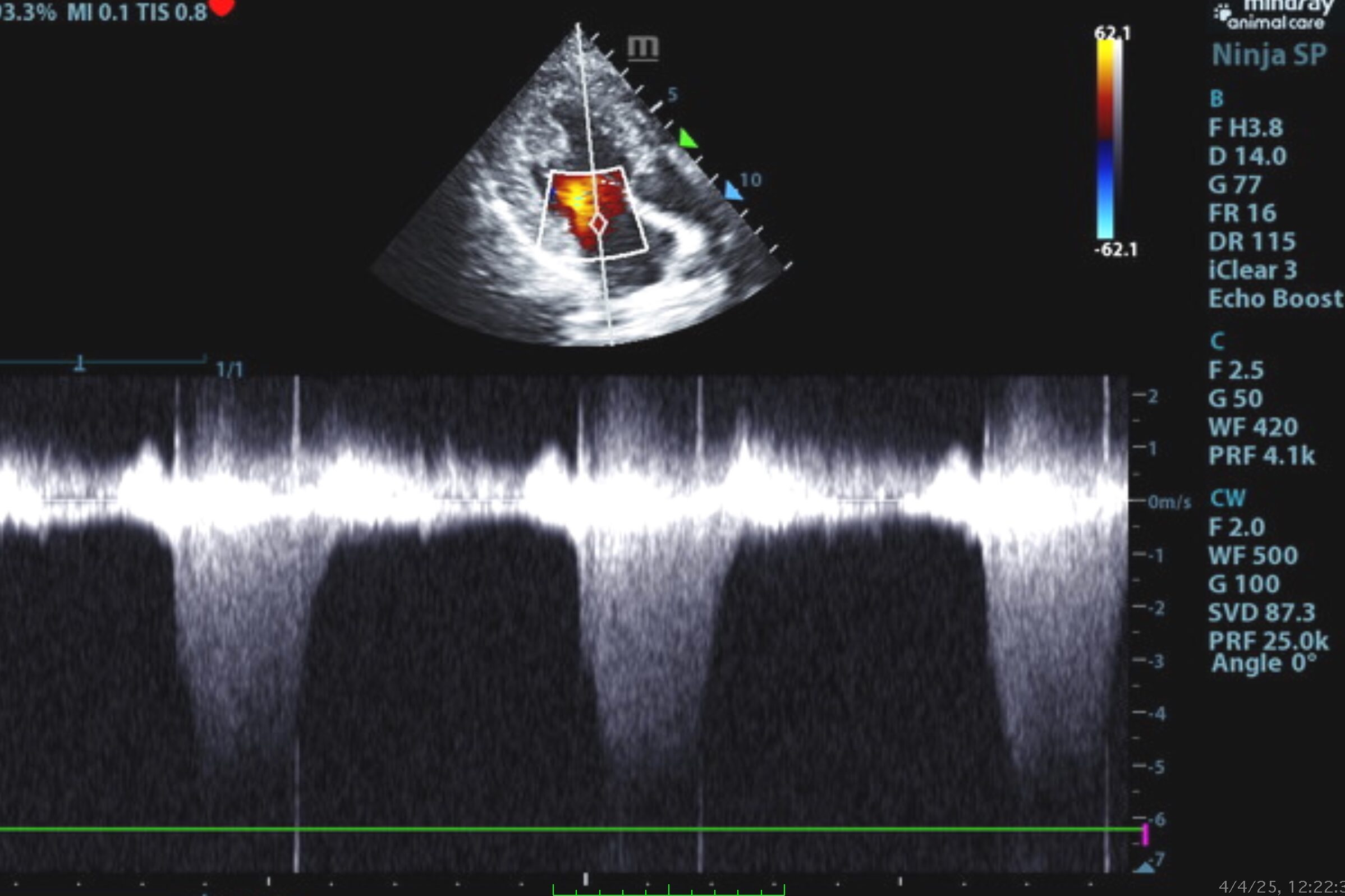
LA evaluation. The mitral valve was vegetative and thickened, primarily the anterior leaflet, yet this
would be more consistent with endocardiosis. Mitral valve insufficiency was noted and measured 5.6
m/sec. The left ventricle presented thicknesses with linear contour and was not dilated nor restricted.
The myocardium presented normal echogenicity without subjective evidence of significant fibrotic or
ischemic disease. Contractility of the ventricular walls was adequate and in normal range for this
patient evidenced by the fractional shortening measurement and subjective evaluation of the different
regions of the myocardium. The aortic valve presented vegetative leaflets strongly consistent with
endocarditis. Aortic insufficiency was noted and measured 6.0 m/sec. The right atrium and auricle
revealed normal size, structure and content. No evidence of masses was noted. Tricuspid valvular
assessment demonstrated adequate linear morphology and kinesis. The right ventricle was of normal
size (1/3 diameter of LV), chordae structure, myocardial echogenicity and thickness. Pulmonary
outflow tract assessment revealed normal valve structure, laminar flow, and diameter (approx.1:1
pa/ao ratio). No visible pericardial or free pleura fluid was noted. The cranial mediastinum and
pericardial and extra-cardiac regions were free of masses in the visible window.

ULTRASONOGRAPHIC FINDINGS
- Aortic and mitral insufficiency, no evidence of volume overload.
- Vegetative endocarditis.
- Some level of pancreatitis is likely.
- Right renal infarct.
INTERPRETATION OF THE FINDINGS & FURTHER RECOMMENDATIONS
This patient is likely experiencing underlying vascular events in the kidneys and endocardium/aortic valve. Some level of pancreatitis or history of pancreatitis is likely. Blood culture, Plavix therapy, enrofloxacin, and clindamycin for empirical therapy is recommended. The prednisolone may be suppressing a more significant presentation. Blood pressure measurements are also indicated. Recheck sonogram if the patient is not improving; intensive care may be necessary. If the patient is improving then a recheck echocardiogram is recommended in 2-3 weeks, continuing antibiotic and Plavix protocol for that length of time. Prognosis is guarded.
Patient Outcome:
Patient is doing well post antibiotics and clinically returned to his normal self.
What is Endocarditis in the Aortic Valve?
Aortic valve endocarditis in the canine patient is an uncommon but highly significant condition involving microbial infection of the endothelial surface of the aortic valve, most commonly due to bacteremia from sources such as urinary tract infections, periodontal disease, or invasive procedures [MacDonald & Chomel, 2023]. The pathogenesis involves endothelial injury, followed by bacterial adherence and the formation of vegetative lesions composed of fibrin, platelets, and colonies of microorganisms [Sykes et al., 2014]. These vegetations can cause significant disruption to normal valve function, leading to aortic insufficiency, volume overload of the left ventricle, and eventual development of left-sided congestive heart failure [MacDonald & Chomel, 2023]. Additionally, septic emboli may disseminate from the valve to distant organs, contributing to multi-systemic complications such as renal infarcts, polyarthritis, and central nervous system involvement [Buchanan, 2000; Sykes et al., 2014]. Without prompt and aggressive treatment—typically requiring prolonged bactericidal antibiotic therapy, often guided by blood culture and sensitivity—the condition carries a guarded to poor prognosis [MacDonald & Chomel, 2023; Sykes et al., 2014]. Early identification and intervention are essential to mitigating irreversible cardiovascular damage and systemic sequelae.
In this case, antibiotic therapy was initiated promptly to address suspected infective endocarditis, targeting likely bacterial pathogens based on clinical presentation and previous culture results. Additionally, a Plavix (clopidogrel) protocol was recommended by specialist Dr. Eric Lindquist to reduce the risk of thromboembolic events secondary to valvular vegetation or endothelial damage. Anti-platelet therapy is particularly important in cases with aortic valve involvement, given the high risk of embolization to critical organs. The combination of targeted antimicrobial treatment and antithrombotic support aims to control infection, preserve cardiac function, and prevent systemic complications.
Citations:
- Buchanan, J.W. (2000). Endocarditis. Textbook of Veterinary Internal Medicine, 5th ed., Ettinger & Feldman (Eds.), W.B. Saunders.
- MacDonald, K.A., & Chomel, B.B. (2023). Infective endocarditis in dogs: Diagnostic challenges and current recommendations. Journal of Veterinary Cardiology, 45, 1–15.
- Sykes, J.E., Kittleson, M.D., Chomel, B.B., & MacDonald, K.A. (2014). Clinicopathologic findings and outcome in dogs with infective endocarditis: 71 cases (1992–2005). Journal of the American Veterinary Medical Association, 234(4), 486–494.

Looking to enhance the range of your ultrasound diagnostic efficiency?
