
While working up a patient with chronic otitis, Dr. Schiess of Rockaway Animal Hospital saw concerns that prompted a deeper look. To further evaluate, the case was referred to the SonoPath Imaging Center in Andover, New Jersey for advanced CT imaging. The CT study was reviewed by radiologist Tilde Rodrigues Froes, DMV, MSc., Dr. Med. Vet., Dipl. CBraRVet, whose interpretation helped clarify the underlying pathology and guided the recommendation for surgical treatment, which turned a frustrating, chronic condition into a clear plan forward with a surgical referral to Oradell Animal Hospital.

The patient was seen by his regular veterinarian for a neuter and itchy ears. A large amount of brown discharge was found. Ear mite swab was negative. Ear cytology revealed cocci. The patient was treated with ear medications which helped the itching but did not resolve the problem. At recheck, a sedated ear exam, ear culture, and flush was performed. The sedated otoscopic exam allowed the rDVM to visualize bilateral macerated tissue within each canal which bled easily when cleaned. Ear culture results identified Staphylococcus felis and Pasteurella dagmatis susceptible to amoxicillin with clavulanic acid. The patient was referred to the Sonopath Imaging Center for a CT scan to evaluate the ear canals and suspected polyps.
CBC Hct 55.6% (30.3-52.3) High
Chem K+ 3.2 (3.5-5.8) Low
A pre- and post-contrast CT study of the head are provided for review totaling 2 series. One pre-contrast series of the head bone algorithm. One post-contrast series of the head soft-tissue algorithm.

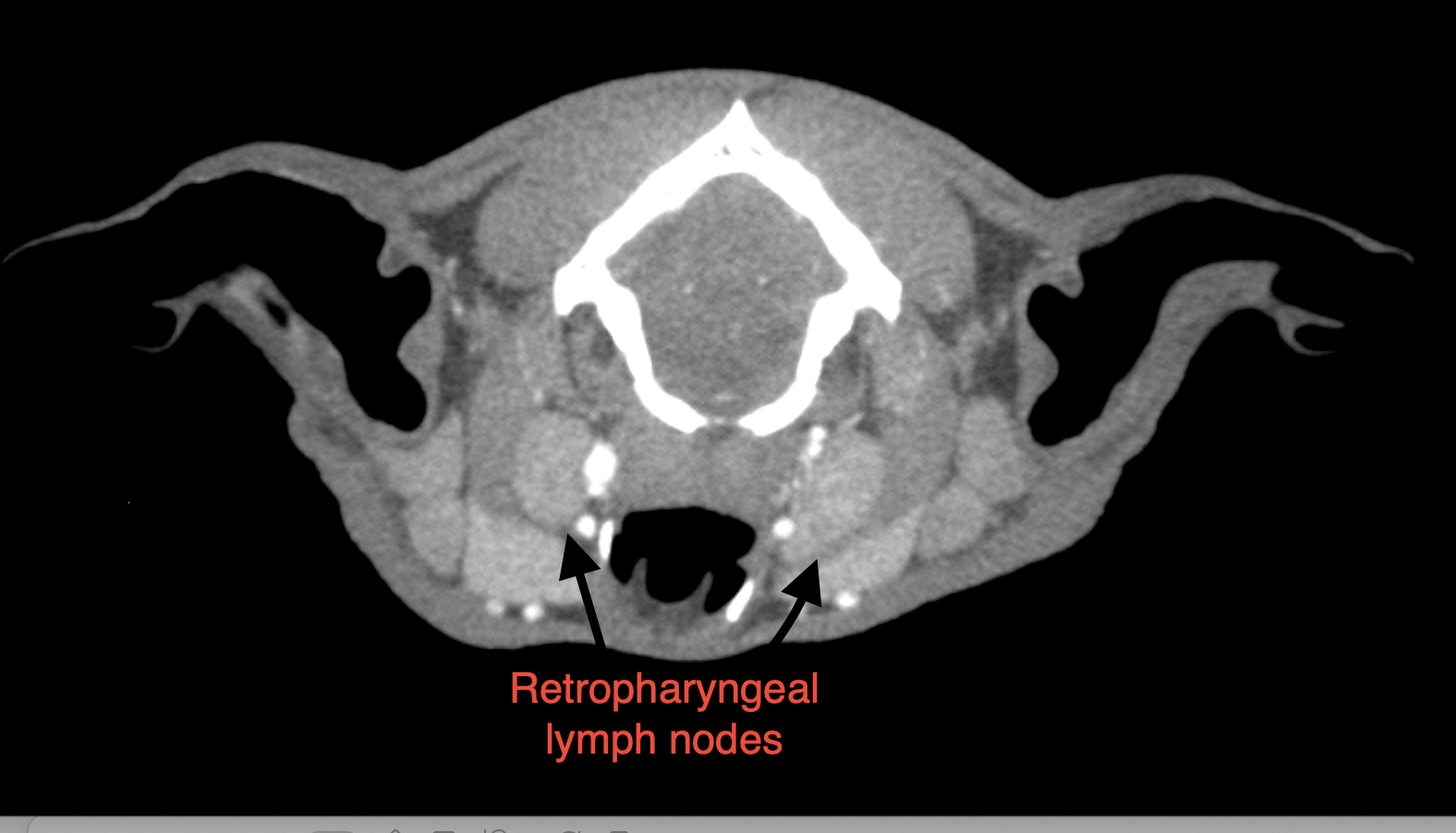
Post-contrast image showing the enlarged retropharyngeal lymph nodes.
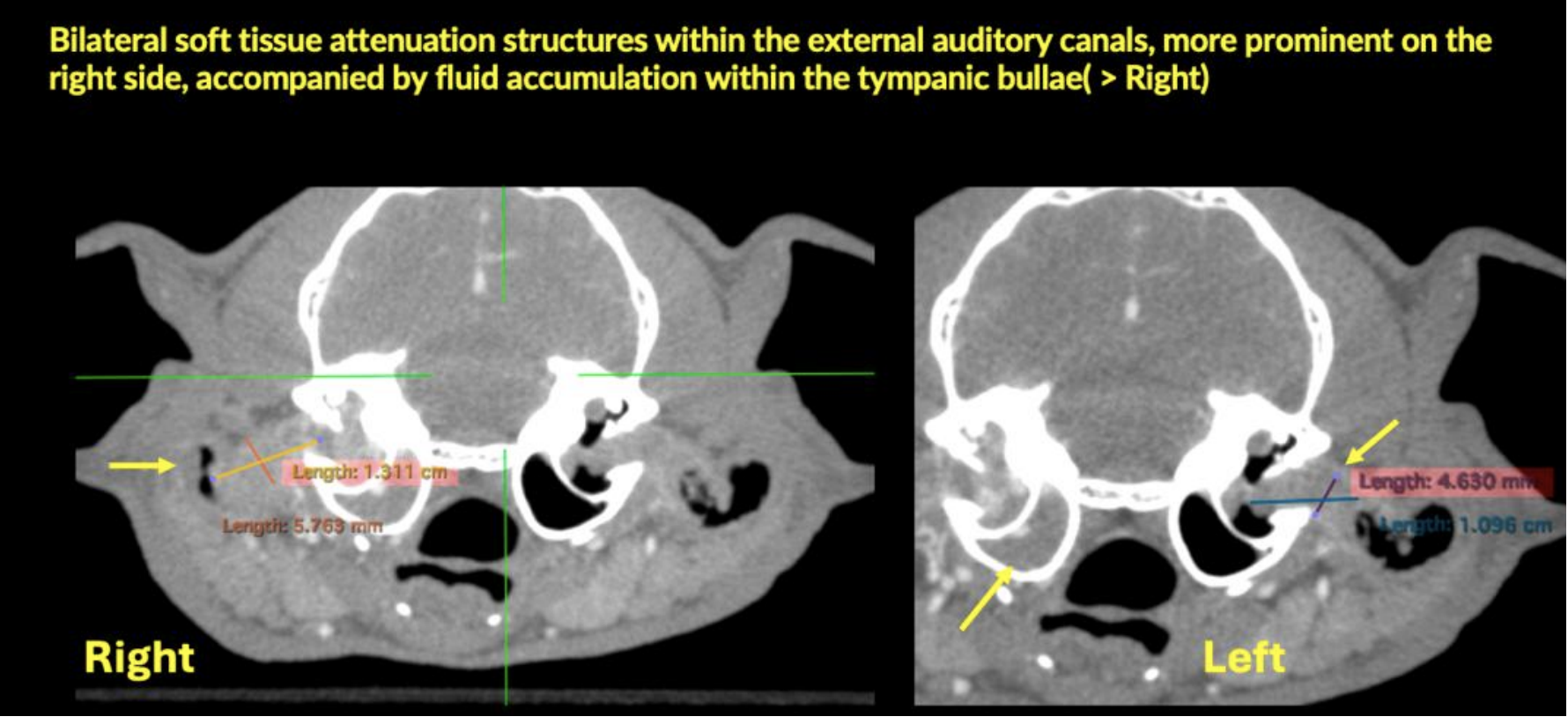
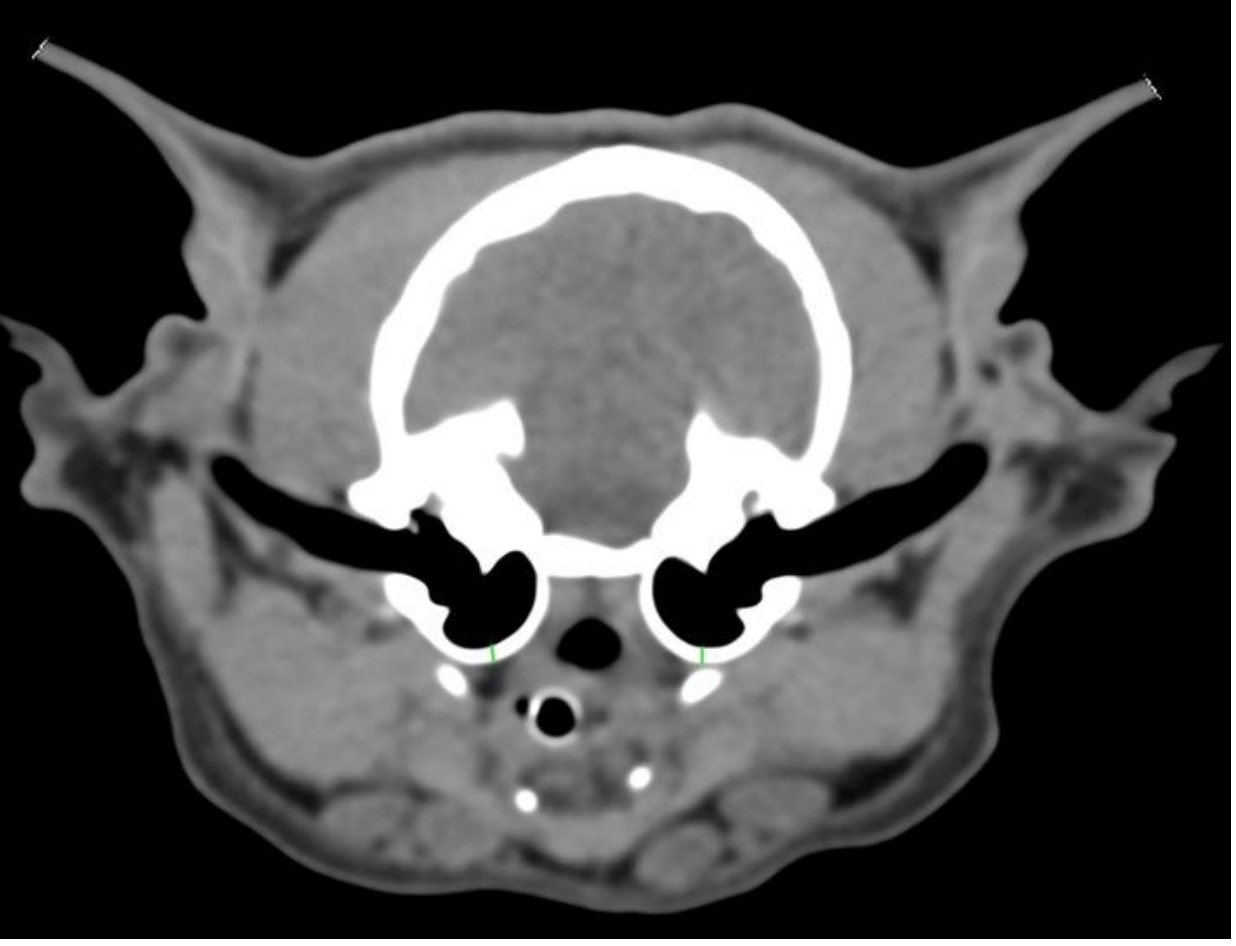
On the left, a CT image showing the measurements of the soft tissue structures within the ear canals.
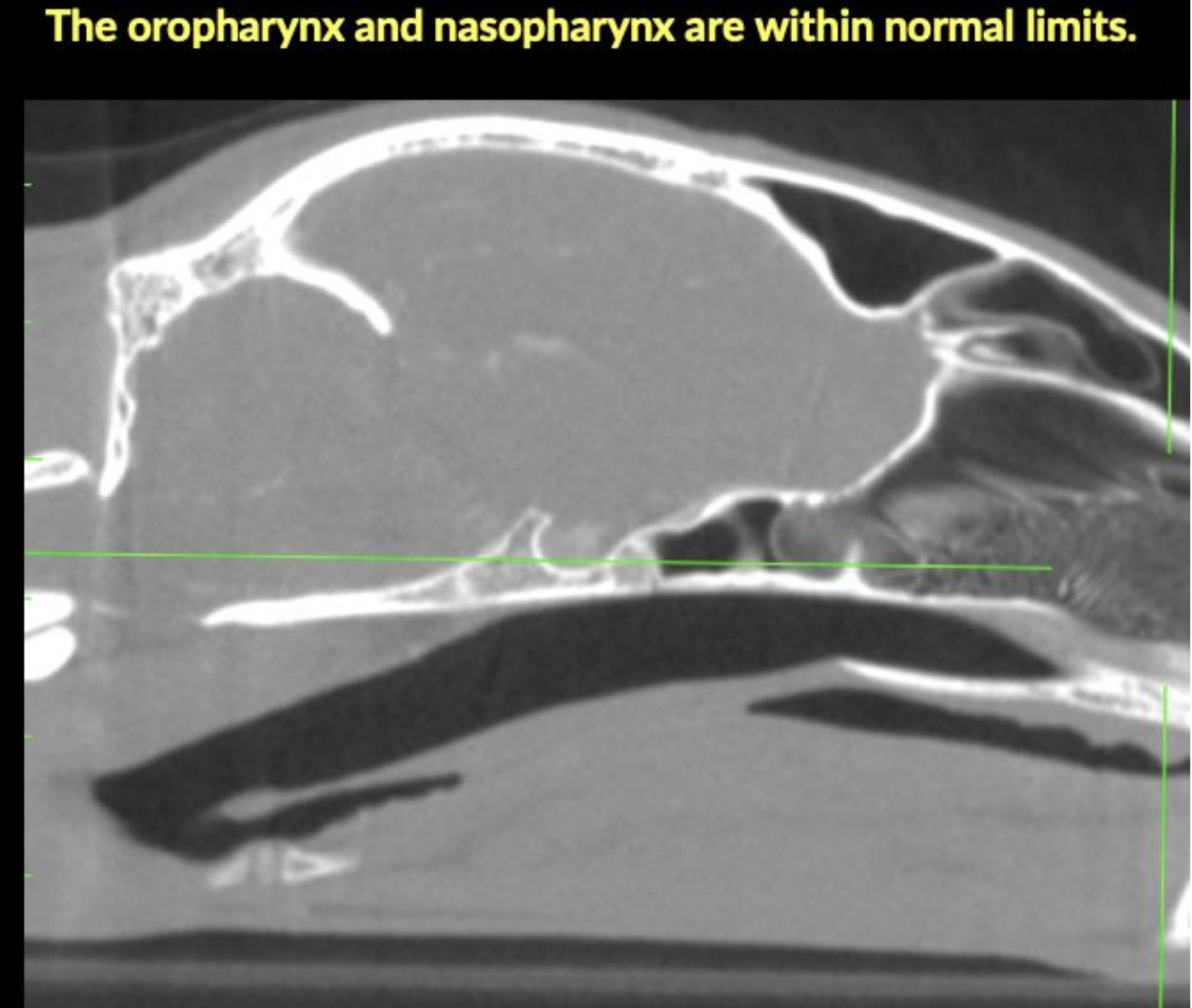
On the right, a sagittal CT image showing the normal oropharynx and nasopharynx.
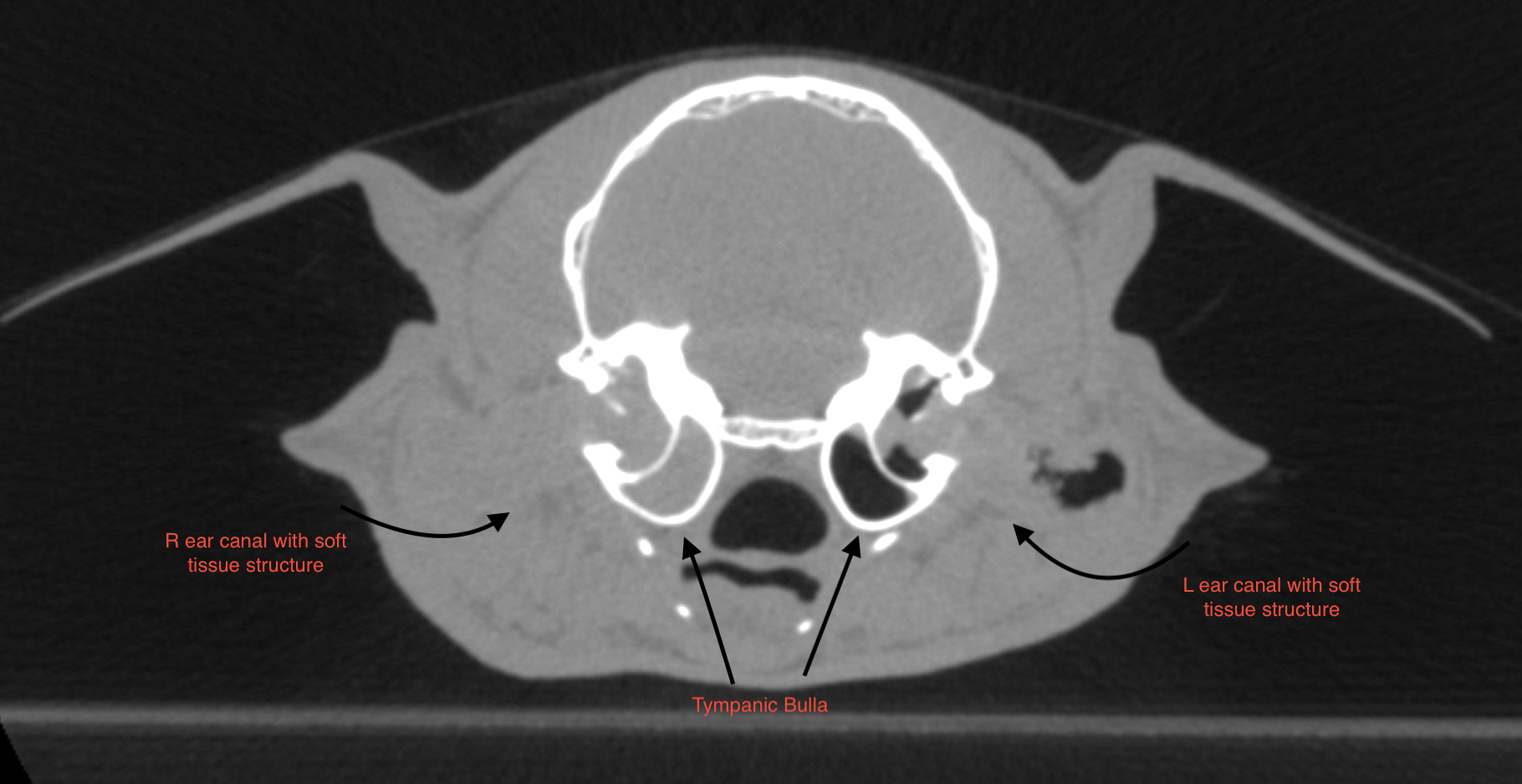
In the right external auditory canal, a large, elongated soft-tissue-attenuation structure with mild peripheral contrast enhancement is observed in the horizontal portion, completely obstructing the lumen and protruding into the region of the tympanic membrane. A small amount of adjacent hypoattenuating fluid is present. The lesion measures approximately 1.3 × 0.57 cm. Moderate hypoattenuating fluid accumulation with peripheral enhancement is noted within the right tympanic bulla, with preservation of the bony wall.
In the left external auditory canal, a moderately sized, elongated soft-tissue–attenuation structure with contrast enhancement is present in the horizontal portion, smaller compared with the right side, and protruding into the region of the tympanic membrane.
Mild adjacent hypoattenuating fluid retention is also observed. The lesion measures approximately 1.0 × 0.46 cm. A discrete amount of hypoattenuating fluid is present within the left tympanic bulla, with preservation of the bony wall.
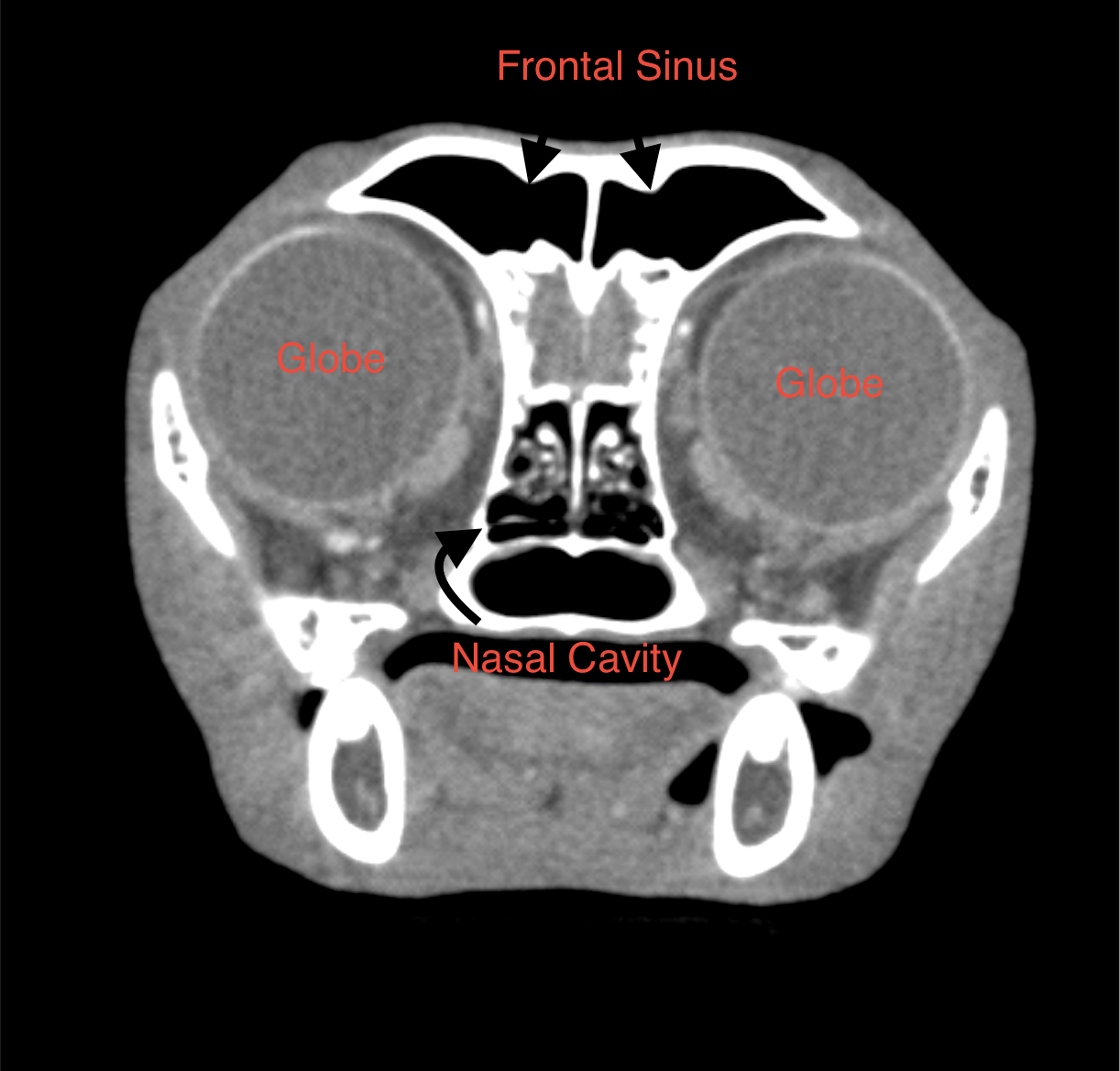
The nasal cavities and frontal sinuses are within normal limits. The oropharynx and nasopharynx are within normal limits. The regional lymph nodes, medial and lateral retropharyngeal are moderately enlarged. The mandibular lymph nodes are within normal limits. The globes, retrobulbar spaces, and brain appear within normal limits.
All teeth are within normal limits. The temporomandibular joints are bilaterally congruent. The mandibular salivary, parotid, zygomatic, and thyroid glands are unremarkable.
• Right external auditory canal exhibits a large soft-tissue–attenuation structure with peripheral contrast enhancement, obstructing the lumen, associated with fluid in the right tympanic bulla. Differential diagnoses include aural polyp, inflammatory lesion, concurrent otitis media, or fluid retention.
• Left external auditory canal exhibits a large soft-tissue–attenuation structure, associated with mild fluid retention and discrete fluid in the left tympanic bulla. Differential diagnoses include aural polyp, inflammatory lesion, and discrete fluid retention within the ipsilateral tympanic bulla.
• Moderate enlargement of the medial and lateral retropharyngeal lymph nodes, reactive lymphadenitis.
The tomographic findings reveal bilateral soft-tissue–attenuation structures within the external auditory canals, more prominent on the right side, accompanied by fluid accumulation within the tympanic bullae (> right).
These findings indicate, as primary differential diagnoses, an aural polyp, inflammatory lesion, concurrent otitis media, or bullae fluid retention.
These findings correlate with the patient’s clinical history of a recurrent otitis externa.
Given the failure of previous medical management and the imaging appearance, surgical intervention with polyp removal and/or debulking via otoscopy is the suggested recommendation. Histopathological evaluation of the excised tissue is advised to confirm the diagnosis.
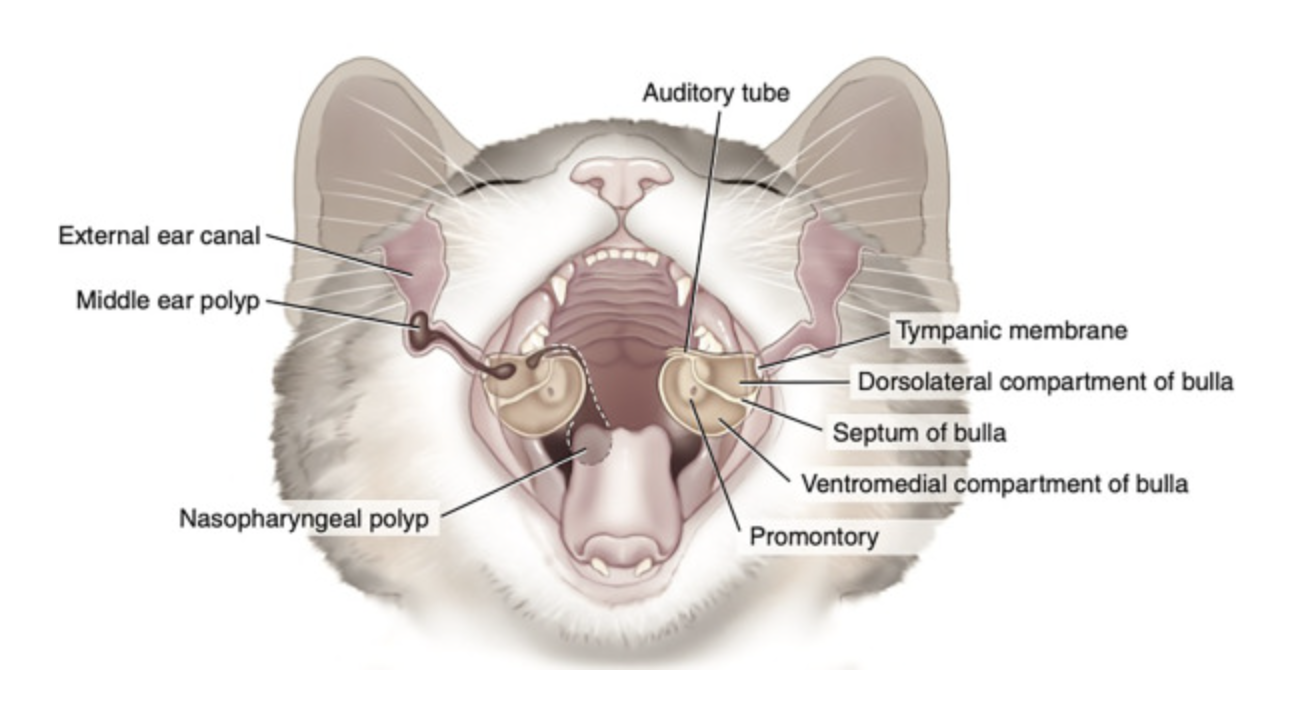
Feline inflammatory aural polyps (IP) are benign, pedunculated growths usually arising from the epithelial lining of the tympanic cavity. They can extend either through the tympanum into the horizontal ear canal or down through the auditory tube into the nasopharynx. They can be unilateral or bilateral.
They tend to occur in younger cats and are rarely seen in dogs. The exact cause is unknown. A genetic component and chronic inflammation due to an infectious cause are theorized.
Cats with nasopharyngeal polyps typically present with upper respiratory signs like stertor, sneezing, and nasal discharge due to secondary bacterial infections. Cats with polyps in the external or middle ear typically have signs of otitis media or interna and possibly neurologic signs such as Horner’s syndrome.
An otoscopic exam and a nasopharyngeal exam using a spay hook to pull the soft palate forward can be used to identify the polyps. Advanced imaging using CT or MRI is the gold standard for evaluation of bilateral polyps and polyps confined to the tympanic bulla.
Traction/avulsion and ventral bulla osteotomy are the most common methods used to remove nasopharyngeal and aural polyps. Histopathology is then recommended to confirm neoplasia is not present.
The patient was referred to Oradell Animal Hospital for dermatology and surgical consult.
Use The Guide’s color-coded chapter tabs to make jumping to the section you need easy.
Are you like us and dog-ear your favorite pages?
That’s true medicine from the inside out!
When should you pick up the probe or schedule a CT? Learn in your own time online with Dr. Eric Lindquist as he presents this one-hour CE lecture with discussion of the differences and benefits of CT and ultrasound, as well as the combined benefit for patients. Lifetime course access only $49.99.
Advanced diagnostic imaging doesn’t have to mean long referrals or distant specialty centers. The SonoPath Imaging Center, located in the heart of Andover, New Jersey, offers advanced diagnostics designed to support you and elevate the care you provide your patients, so exceptional care stays close to home. We look forward to supporting you soon!


References
1. Srisowanna N, Darawiroj D, Choisunirachon N, et al. Morphological and Morphometric Variations of the Tympanic Bulla Between Domestic Shorthair and Brachycephalic Cats Utilizing Computed Tomography. The Thai Journal of Veterinary Medicine 2024;54:175–182.
2. Tobón Restrepo M, Espada Y, Aguilar A, et al. Anatomic, computed tomographic, and ultrasonographic assessment of the lymph nodes in presumed healthy adult cats: The head, neck, thorax, and forelimb. Journal of Anatomy 2021;239:264–281.
3. Hoppers SE, May ER, Frank LA. Feline bilateral inflammatory aural polyps: a descriptive retrospective study. Veterinary Dermatology 2020;31:385-e102.
4. Orsini J. Comparative Veterinary Anatomy. Elsevier; 2022. Available at: https://linkinghub.elsevier.com/retrieve/pii/C20160010033. Accessed January 26, 2026.