
Referring DVM: Dr. John Andalaft at Animal Care Center of North Jersey
CT Scan: Sonopath Imaging Center
Specialist (Radiology): Sebastian Jawinski, German Board-Certified Vet Specialist in Diagnostic Imaging
Surgical Referral: Red Bank Veterinary Hospital

An 11-year-old female spayed Maltese presented for a 6-month history of intermittent vomiting and diarrhea, lethargy, and urinary accidents in the house. The patient is fed C/D diet for previously diagnosed urinary bladder calculi. Bloodwork showed elevated PTH and iCa. A CT scan was recommended to screen for a parathyroid tumor. The results are below.
Chemistry:
Calcium 15.1 (8.9–11.4 mg/dL) HIGH
ALKP 569 (5–131 IU/L) HIGH
Vitamin D/Calcium panel:
Vitamin D 82 (112–366 nmol/L) LOW
Intact PTH 24.4 (1.1–10.6 pmol/L) HIGH
Ionized Ca 1.8 (1.25–1.45 mmol/L) HIGH
Calcium 15.4 (8.9–11.4 mg/dL) HIGH
The results of this profile are consistent with a diagnosis of primary hyperparathyroidism. The concentration of 25 hydroxyvitamin D is decreased and is not suggestive of excessive dietary intake of vitamin D as the cause of hypercalcemia.
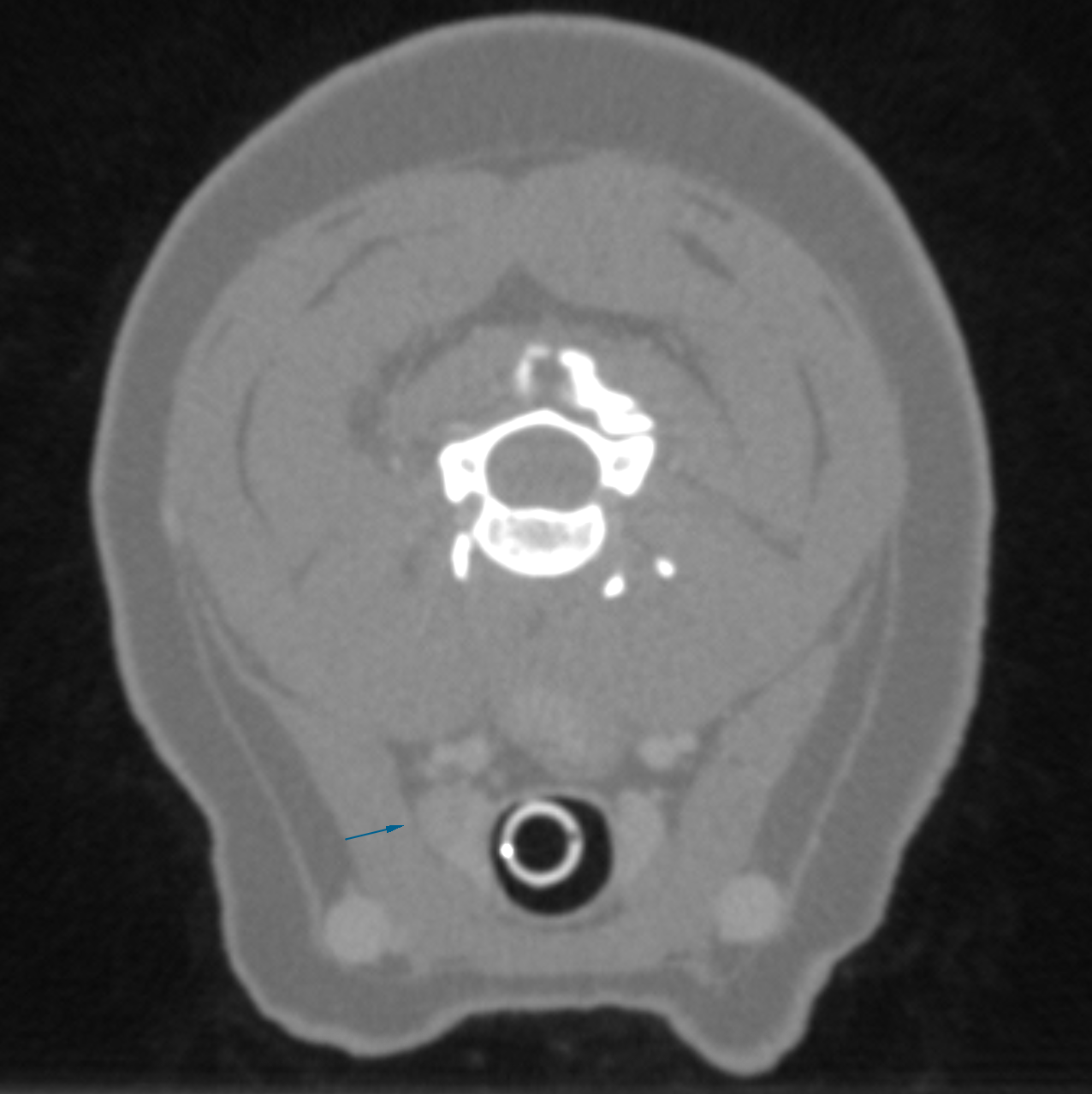
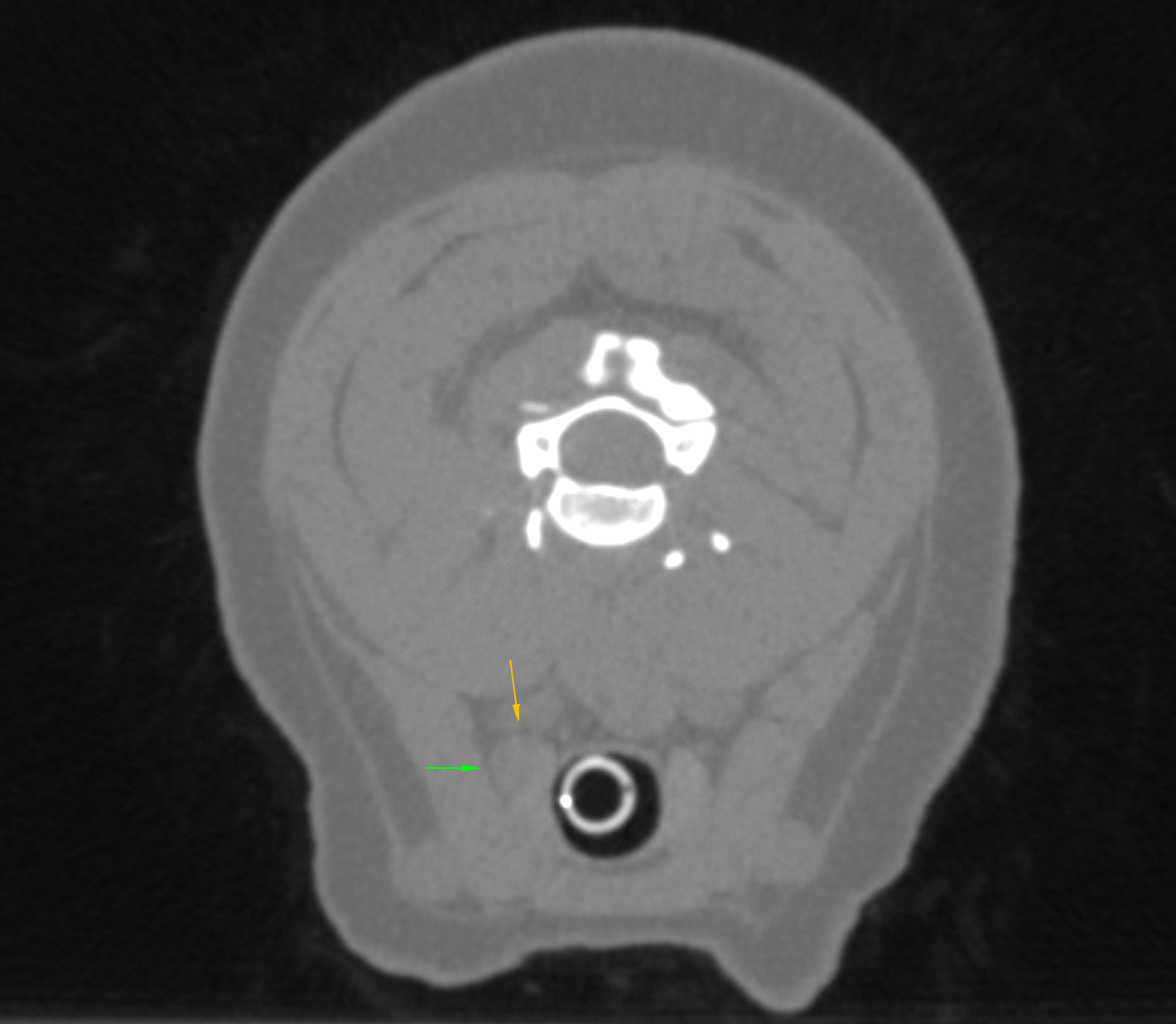
Video showing the CT precontrast at the level of the parathyroid nodule
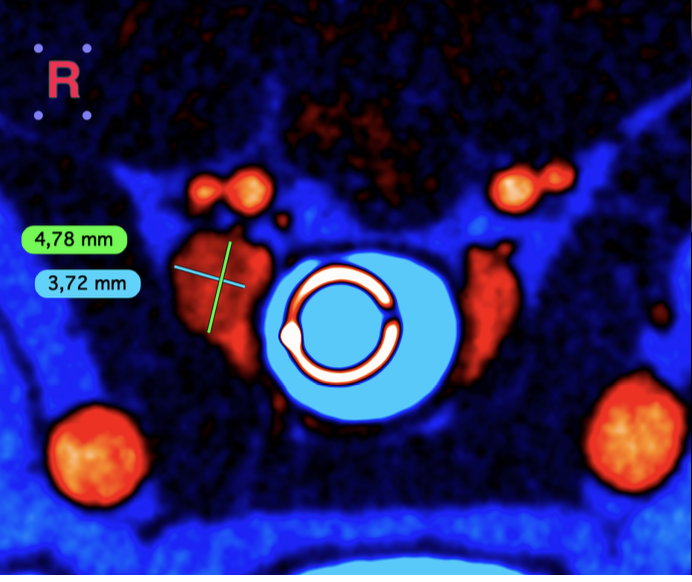
The right thyroid gland shows a nodular lesion of 6.6 x 3.9 x 4.8 mm being mildly inhomogeneous after contrast application. Protrusion of thyroid capsule is detected. The direct periphery does not show signs of invasive or aggressive behavior. The thyroid gland on the left side is inconspicuous. Trachea and esophagus are unremarkable as well as the interfascial planes.
The retropharyngeal lymph nodes are symmetrical and without particular findings. The soft tissues of the neck are inconspicuous apart from that. The displayed parts of the thoracic inlet and the cranial mediastinum are normal.
Suspected neoplastic lesion right caudal/internal parathyroid gland.
The changes of the right thyroid gland do match with the blood results and are suspicious for a
neoplastic lesion of the right internal/caudal parathyroid gland. Diameters that exceed 4 mm are more likely to be neoplastic than hyperplastic. The unilateral finding would underline the assumption of neoplasia. Differentials include adenoma/adenomatous hyperplasia and adenocarcinoma. CT cannot differentiate benign from malignant lesions in the absence of an aggressive/invasive growth.
Ultrasound-guided FNA could be performed next. With the unilateral finding heat/alcohol ablation or surgical resection should be discussed.
Primary hyperparathyroidism (PHPT) in the dog is caused by excessive synthesis and secretion of parathyroid hormone (PTH) by abnormal chief cells of the parathyroid gland. This may be due to a parathyroid adenoma (85%), carcinoma (5.4%), or hyperplasia (12.4%). The excess secretion of PTH causes an increase in serum calcium due to mobilization from bone and resorption from the kidneys. Dogs with hypercalcemia usually present with PU/PD, lethargy, gastrointestinal signs, and changes in appetite; some have urolithiasis. Diagnosis of PHPT is made based on a persistently high ionized calcium and a normal or high PTH concentration, a serum PTHrP concentration of 0 pmol/L, serum phosphorus concentration within or less than the reference interval, ultrasonographic identification of a nodule on a parathyroid or thyroid gland, and exclusion of other causes of hypercalcemia, with no evidence of renal disease.
Ultrasound is typically used as a screening tool to identify abnormal parathyroid glands. Ultrasound accuracy can be limited by factors such as minimal gland enlargement, poor delineation of the gland’s borders, and the skill of the ultrasonographer. CT scan has superior tissue resolution, but the parathyroid glands are still hard to visualize due to size. CT with contrast enhancement was a useful tool in diagnosing parathyroid disease. Although CT scan was more accurate in identifying diseased parathyroid tissue, surgical exploration was able to identify additional nodules that the CT scan did not identify.
Parathyroidectomy is the current treatment of choice for PHPT and has an overall cure rate of approximately 95%. Minimally invasive techniques such as ultrasound-guided ethanol ablation or heat ablation have been described but have a lower success rate of 70%–90%.1 2 3 4
The patient was transferred to Red Bank Veterinary Hospital and given the options of surgical removal or ethanol ablation of the abnormal parathyroid gland. The owner elected to pursue parathyroidectomy as well as cystotomy to remove the urinary bladder calculi. The patient did well after surgery. The patient’s ionized calcium was within normal limits up to 2 days post surgery, then became mildly hypocalcemic, and returned to within normal limits 2 weeks post op.
Stone Analysis: Calcium Oxalate calculi
Histopathology: Parathyroid adenoma
The Broad Scope of Ultrasound
1 RACE-approved CE credit ($69.00)
This on-demand lecture discusses the differences and benefits of CT and ultrasound, as well as the combined benefit for patients. Case studies with sampling and cytologic findings will be presented and discussed in this RACE-approved CE course.
Basic Ultrasound Image Optimization
1 RACE-approved CE credit ($49.00)
Our newly updated video and keynote for this 1-hour course covers an introductory look at the main control settings of an ultrasound system, and how to utilize them in both pre- and post- processing to optimize ultrasound images for proper diagnostic purposes.
Scan the QR codes at the start of each chapter for in-depth case reviews from authors Dr. Peter Modler and Dr. Eric Lindquist!
Your Go-To Rereference for everything after the probe.
References
1. Guttin T, Knox VW, Diroff JS. Outcomes for dogs with primary hyperparathyroidism following treatment with percutaneous ultrasound-guided ethanol ablation of presumed functional parathyroid nodules: 27 cases (2008–2011). JAVMA 2015;247:771–777.
2. Feldman EC, Hoar B, Pollard R, et al. Pretreatment clinical and laboratory findings in dogs with primary hyperparathyroidism: 210 cases (1987-2004). J Am Vet Med Assoc 2005;227:756–761.
3. Young KM, Degner DA. Surgical description and outcome of ultrasound-guided minimally invasive parathyroidectomy in 50 dogs with primary hyperparathyroidism. Veterinary Surgery 2023;52:18–25.4. Boszko M, Burgess R, Paek M. Prospective Study on the Agreement of Computed Tomography and Surgery in the Identification of Parathyroid Pathology. Veterinary Radiology & Ultrasound 2025;66:e70044.