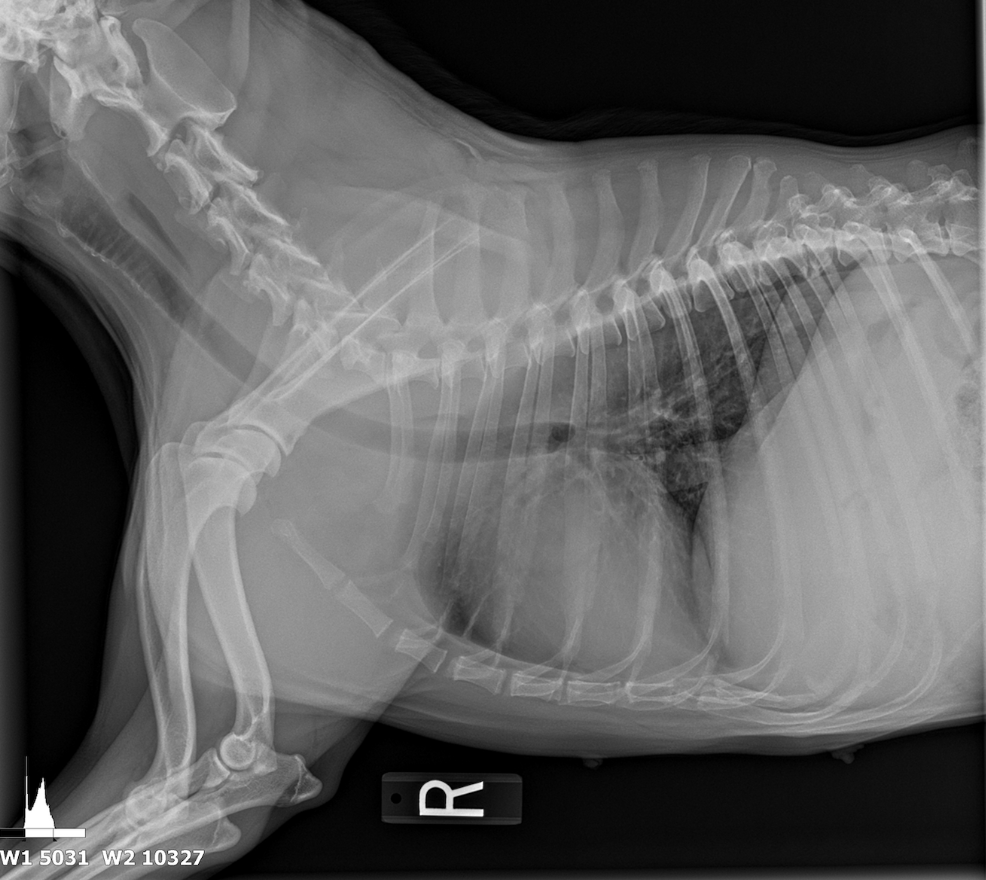
The patient was referred from another veterinary clinic for advanced imaging following the identification of a suspected abdominal mass on radiographs. Ultrasonographic evaluation revealed a splenic mass consistent with an abscess, from which purulent fluid was aspirated and drained. A splenectomy was scheduled for later the same day.
At presentation, the patient was lethargic and febrile. Physical examination and diagnostic testing revealed multiple abnormalities. The complete blood count (CBC) demonstrated a non-regenerative anemia (hematocrit 25%) and marked leukocytosis characterized by neutrophilia (neutrophil count: 21,000/µL). Serum chemistry showed elevated alkaline phosphatase (ALP) and increased globulin concentrations. A 4DX test returned negative results, and a coccidioidomycosis titer was pending at the time of reporting.
A heartfelt thank-you goes to Dr. Gudrun Gunther, SDEP® Certified Clinical Sonographer, and the team at New Frontier Animal Medical Center for their excellent case management and imaging. Dr. Gunther’s dedication to continuous learning through SonoPath’s hands-on labs and her mastery of the SDEP® protocol were instrumental in identifying the splenic abscess and guiding timely surgical intervention. Special thanks as well to Dr. Eric Lindquist for his expert interpretation and for developing the SDEP® Protocol, a system that continues to advance diagnostic precision and save lives across practices every day.



ULTRASONOGRAPHIC EXAMINATION OF THE ABDOMEN:
Urinary System:
The urinary bladder, trigone, and pelvic urethra presented normal thicknesses and normal tone. The ureters were not visible which is normal. A trace amount of sediment was noted in the bladder. No evidence of inflammatory or neoplastic changes was noted. Ureteral papillae were normal. The kidneys revealed normal size and structure, corticomedullary definition and ratio for this age. The cortices presented largely uniform texture with normal echogenic relationship to liver and spleen. Medullary structure differed distinctly from the cortex and no evidence of pelvic dilation was present. The capsules were acceptably uniform without significant irregularities. The left kidney measured 7.0 cm.
Adrenal Glands:
Both adrenal glands were visualized and recognized as having normal shape, size, position and echogenicity for this breed. The phrenic vasculature, glandular echogenicity and detail were unremarkable. Capsule, cortex, and medullary definition were normal for this age patient. The left adrenal gland measured 2.6 x 0.58 cm at the caudal pole and 0.46 cm at the cranial pole. The right adrenal gland measured 2.7 x 1.56 cm at the cranial pole and 0.52 cm at the caudal pole.
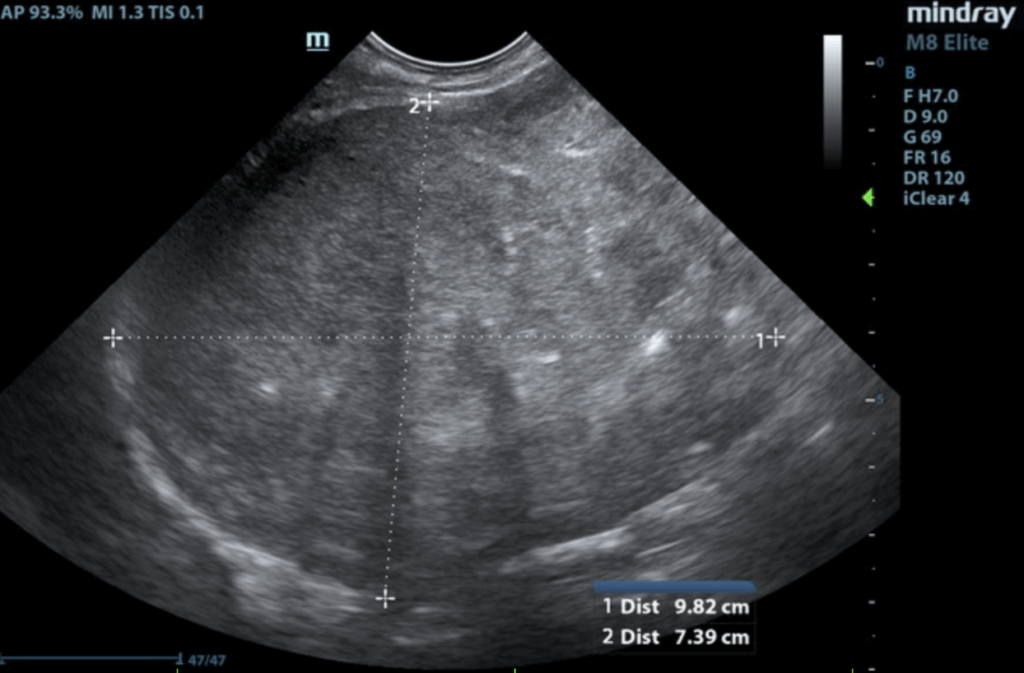
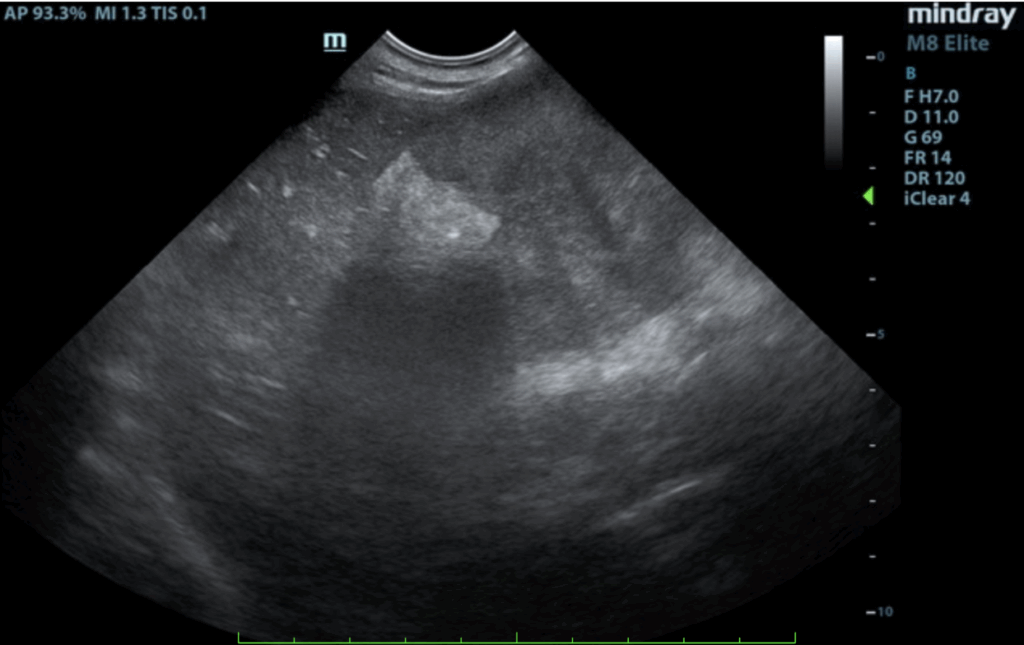
Spleen:
The spleen revealed an expansive parenchymal mass that measured 10+ cm without evidence of cavitation. Hyperechoic fat was noted around the spleen. This is consistent with inflammation.
Liver:
The liver images submitted revealed subjectively normal liver size, contour, and structure. Parenchymal echogenicity was naturally coarse and hypoechoic to the spleen. Vascular and biliary tracts were of normal volume with no evidence of congestion. The gallbladder presented acceptably thin walls with primarily anechoic content. The cystic and common bile ducts were normal. No pathological hepatic lymphadenopathy was evident. No overt structural evidence of inflammatory, infiltrative or regenerative pathology was evident.
Gastrointestinal:
Examination of the gastrointestinal tract revealed a stomach and intestine free of stasis, of normal wall thickness, acceptable curvilinear mural detail, and peristaltic activity. Small and large intestine demonstrated normal luminal chyme and stool consistency respectively. No obstructive or overt infiltrative disease was noted. No associated abnormal lymphatic activity was noted.
Pancreas:
The base and limbs of the pancreas were observed to be largely isoechoic to surrounding omental fat. Pancreatic duct and capsular contour were acceptably normal and parenchyma respected normal curvilinear patterns. No overt evidence of active inflammatory or neoplastic disease was noted.
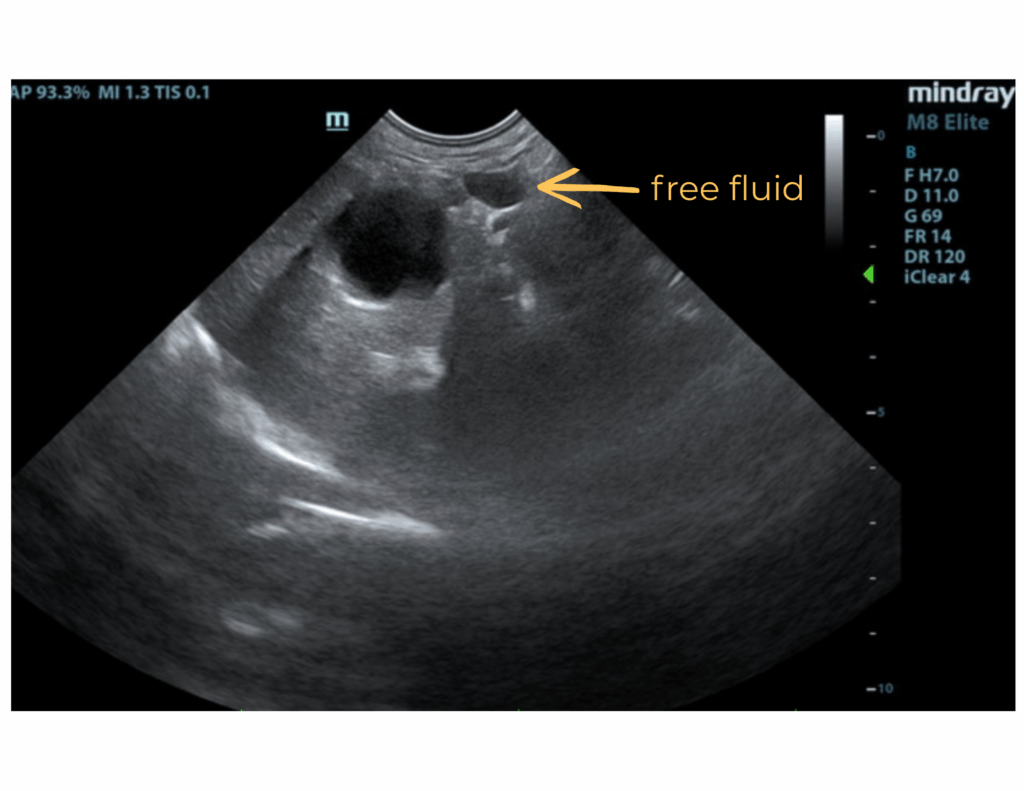
Free Abdomen:
A slight amount of free fluid was noted.
ULTRASONOGRAPHIC FINDINGS:
- Splenic mass.
- Free fluid.
INTERPRETATION OF THE FINDINGS & FURTHER RECOMMENDATIONS:
There was no obvious evidence of metastatic disease. Proactive splenectomy, liver inspection and biopsy was indicated. Rapid echocardiogram was recommended if not already performed to ensure that metastatic disease was not present. Differentials included benign hyperplasia, hemangiosarcoma and round cell neoplasia. However, the mass was highly precarious and at risk for rupture.
Discussion with Surgery and Patient Outcome:
The patient underwent a splenectomy and the purulent fluid was cultured.
Culture Results: Staphylococcus pseudointermedius which was susceptible to amoxicillin/clavulanate and enrofloxacin, started after surgery. No need for additional treatment.


Clinically, the patient improved significantly within day of the splenectomy and was back to normal 4 days post surgery. The patient even gained 5 lb from 7/3 to 7/15 at time of staple removal.
Splenic abscesses are a rare finding in dogs. The etiology of a splenic abscess in a dog is not fully understood. There are only a few documented case reports. Much of the literature on splenic abscesses comes from the human side. It has been mostly seen in immunocompromised patients or due to penetrating foreign bodies and splenic torsion. It is suggested that splenic damage and bacteremia causes necrosis and formation of an abscess in humans. There may be a similar pathogenesis in dogs.
In most of the canine case reports, the patient presented with lethargy, pyrexia, decreased appetite and a mass seen on radiographs or felt on palpation. Bloodwork consistently showed anemia, thrombocytopenia, and leukocytosis with a neutrophilia and an elevated ALKP.
If a splenic abscess is the only abnormality present, then the prognosis appears to be good with early surgical intervention, abdominal lavage, culture and antibiotics.
References:
1. Oyamada T, Nabeta R, Azakami D. A canine case of splenic hemangiosarcoma complicated with infectious splenic abscess. Vet Res Forum 2022;13:451–454.
2. Ginel, P.J. Diffuse splenomegaly caused by splenic abscessation in a dog. The Veterinary Record. Ovid. 2001; 149; 327-329
3. Abdellatif A, Günther C, Peppler C, et al. A rare case of splenic abscess with septic peritonitis in a German shepherd dog. BMC Vet Res 2014;10:201.
4. Rubanick JV, Breiteneicher AH, Thieman-Mankin K. Large-volume pneumoperitoneum and septic peritonitis secondary to splenic abscess rupture in a dog. Can Vet J 2020;61:138–141

Looking to enhance the range of your ultrasound diagnostic efficiency?
