
Meatball presented as a participant in the November 2025 SonoPath Imaging lab. He was brought in by Camp Papillon Animal Rescue in Stroudsburg, PA. At each SonoPath training lab, every animal participant receives a thorough physical exam and a complete abdominal ultrasound and echocardiogram. At this lab he was examined by Dr. Renee Trionfetti. A 5/6 murmur was auscultated. The physical exam was otherwise normal. Because of the murmur, he was not sedated to participate in the training. Instead, he received a complete abdominal ultrasound and echocardiogram performed by Dr. Tam Nolan Mengine for murmur evaluation. Dr. Eric Lindquist interpreted the studies and found severe pulmonic stenosis.
Meatball was referred to the cardiology department at Red Bank Veterinary Hospital where he underwent further evaluation. He ultimately received a balloon valvuloplasty to treat his pulmonic stenosis. The procedure was successful, and he recovered well during his hospitalization.
Specialist: Eric Lindquist, DMV, DABVP
SonoPath Imaging Lab: Renee Trionfetti, DVM; Tam Nolan Mengine, DVM, DABVP
Special Thanks to Red Bank Veterinary Hospital Cardiology Department

US video SDEP® Position 1 short axis heart base showing the abnormal pulmonic valve.
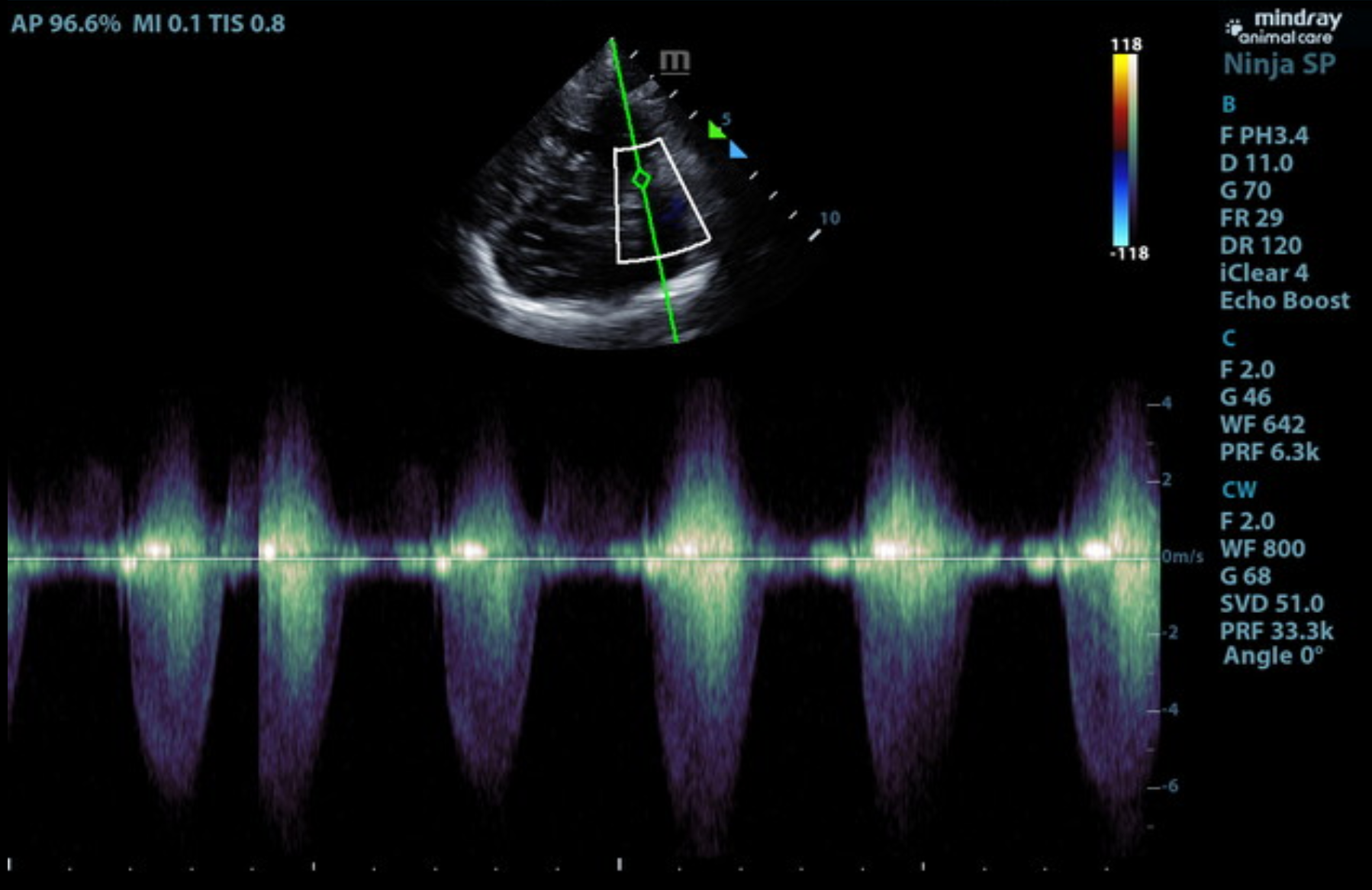
US video SDEP® Position 1 short axis heart base showing the abnormal color flow and decreased diameter through the pulmonic valve and pulmonary artery.
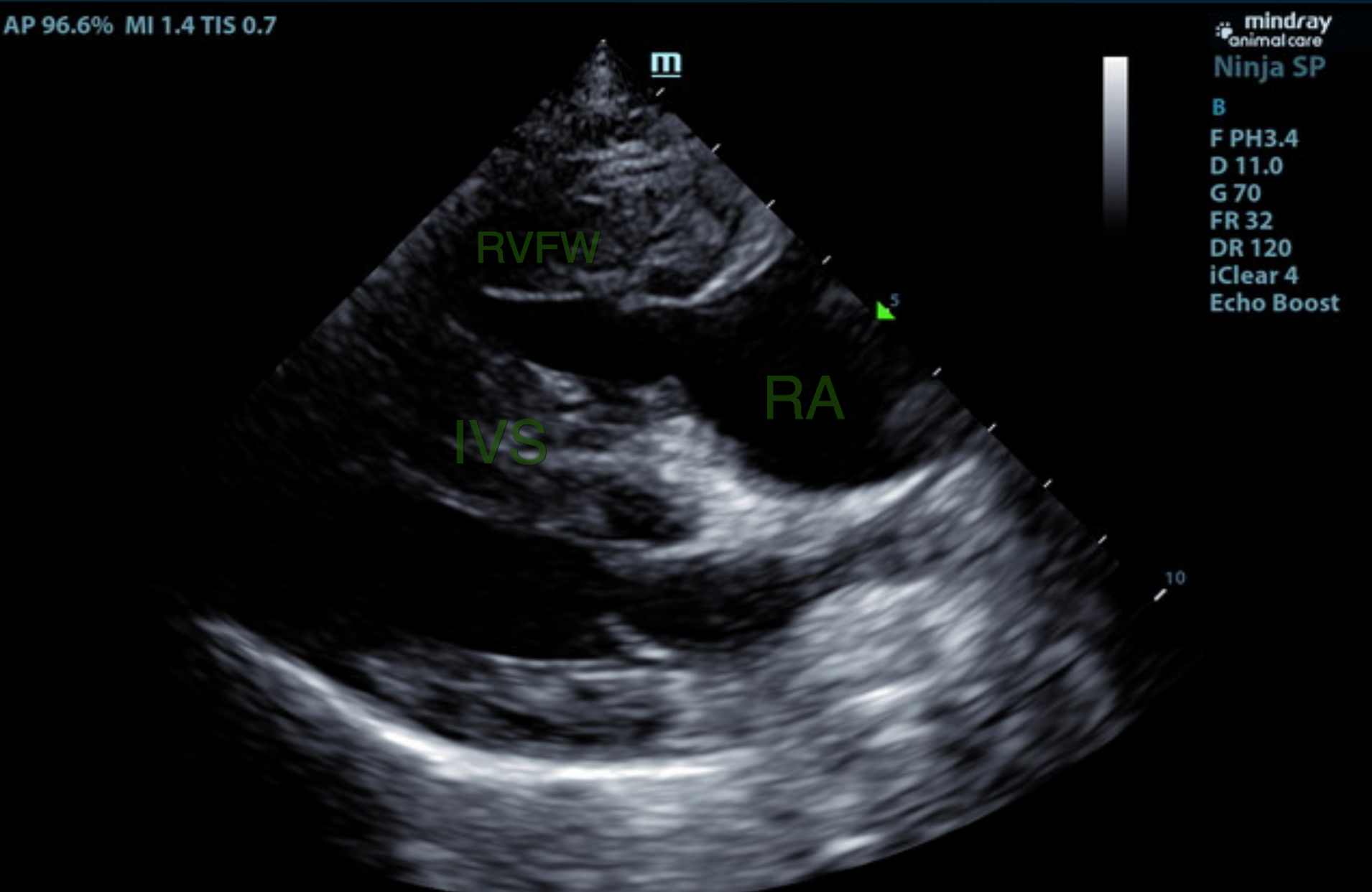
US Video at SDEP® Position 1 showing the right sagittal 4 chamber view of the heart. The right ventricular free wall and interventricular septum are thickened.
The echocardiogram in this patient demonstrated normal left atrial size based on three separate methods of LA evaluation. The cranial and caudal mitral valve leaflets presented normal linear structure, extension in systole, and union in diastole with normal kinesis. The left ventricle presented thicknesses with linear contour and was not dilated nor restricted. The myocardium presented normal echogenicity without subjective evidence of significant fibrotic or ischemic disease. Contractility of the ventricular walls was adequate and in normal range for this patient evidenced by the fractional shortening measurement and subjective evaluation of the different regions of the myocardium. The left ventricular outflow tract demonstrated normal laminar flow and subjective structural integrity. The right atrium and auricle revealed normal size, structure and content. No evidence of masses was noted. Tricuspid valvular assessment demonstrated adequate linear morphology and kinesis. The right ventricle was of normal size (1/3 diameter of LV), chordae structure, myocardial echogenicity and thickness. Severe pulmonic stenosis was noted in this patient. No visible pericardial or free pleura fluid was noted. The cranial mediastinum and pericardial and extra-cardiac regions were free of masses in the visible window.
- Normal Abdomen
- Severe Pulmonic Stenosis
Atenolol is recommended at 12.5 mg (total dose) orally twice a day. Balloon valvuloplasty would be ideal; however, additional assessment may be needed to rule out coronary artery anomaly. There was no evidence of congestive heart failure at this time.
Pulmonic stenosis (PS) is a congenital defect in which the pulmonary valve is narrowed, causing obstruction of the right ventricular outflow tract. PS is one of the most common congenital heart defects seen in dogs. The abnormality and narrowing is commonly found at the valve but can be supravalvular or subvalvular. On physical exam, a loud murmur will be heard and the patient can present with exercise intolerance, syncope, right-sided congestive heart failure, or sudden death.
Echocardiography allows for definitive diagnosis. Echo will typically show right ventricular hypertrophy due to the outflow obstruction at the pulmonic valve. At the pulmonary artery you will typically see thickened, immobile, and, sometimes, fused cusps. A subvalvular ring may also be present. A hypoplastic pulmonary artery or annulus may be present. Post-stenotic dilation occurs in the pulmonary artery. Tricuspid regurgitation may develop and cause right atrial enlargement if severe. On color Doppler there will be turbulent blood flow in the pulmonary artery. On CW Doppler velocity can be evaluated and severity determined. A PA Vmax of > 5 m/sec is considered severe.
Balloon dilation valvuloplasty is the treatment of choice for severe valvular PS. The balloon dilation, if successful, can reduce the pressure in the right ventricle by 50%. Up to 71–80% of dogs treated with balloon valvuloplasty are asymptomatic postoperatively. 1 2 3
“Meatball is doing fabulously in foster, having the time of his life, appears to be recovered. His follow up visit is 07/11/2026 for an echo, the way he is behaving, we believe the surgical intervention was successful!!
Thank you to your team for discovering his problem and all you do for us! We appreciate you!”
– Camp Papillon Animal Rescue in Stroudsburg, PA
Normal Ultrasound Image Library: Echo
On-Demand Image Reference Library
This canine and feline reference library of normal anatomy, standard views, efficiency clips, and age-related sonographic variations in Echo is designed for veterinarians and veterinary technicians who want a reliable visual reference to improve image recognition, scanning consistency, and echocardiographic confidence.
Cardiology Series with Dr. Peter Modler
14 RACE-approved CE credit ($799.00)
Designed for veterinarians seeking a clear, practical understanding of cardiology from the foundational physiology to advanced echocardiographic interpretation and clinical-decision making with SonoPath specialist and SDEP® instructor, Dr. Peter Modler, DVM, Dipl.-Tzt., Specialist German Board of Cardiology
Check out the Curbside Guide chapter “Pulmonic Stenosis & Other Obstructions to Right Ventricular Outlfow” (pg 435–448) to read more about clinical signs, diagnostics, and clinical findings.
The Curbside Guide bridges the gap between “what did I see?” and “what do I do now?” for cases like Meatball’s!
with our new SDEP® Advanced Cardiology lab this November!
If you are comfortable performing routine echo exams, this one is for you!
Designed for advanced veterinary sonographers ready to refine echocardiographic technique, improve diagnostic interpretation, and integrate advanced cardiac pathology into clinical decision-making, SDEP® Advanced Cardiology lab expands beyond image acquisition to focus on the “why” behind cardiac findings!
References
1. Johnson MS, Martin M, Edwards D, et al. Pulmonic stenosis in dogs: balloon dilation improves clinical outcome. J Vet Intern Med 2004;18:656–662.
2. Lucina SB, Sarraff AP, Wolf M, et al. Congenital Heart Disease in Dogs: A Retrospective Study of 95 Cases. Top Companion Anim Med 2021;43:100505.
3. Locatelli C, Spalla I, Domenech O, et al. Pulmonic stenosis in dogs: survival and risk factors in a retrospective cohort of patients. Journal of Small Animal Practice 2013;54:445–452.