
A 15-year-old poodle arrived at Creditview Eglinton Animal Hospital with collapsing episodes that raised concern for seizures versus syncope. Dr. Ghobrial from Creditview Eglinton AH and The Focal Zone’s Kelly Reschny, RVT, moved quickly, performing an echocardiogram and 6-lead ECG using the Beecardia system. The case was promptly reviewed by SonoPath cardiology specialist Dr. Maggie Lamy, who delivered a detailed interpretation and treatment recommendations. These rapid diagnostics helped discern if underlying arrhythmia or pulmonary hypertension was driving the episodes, turning uncertainty into a clear clinical path forward.

The patient presented with a history of acute onset of seizure-like episodes, abdominal discomfort, and decreased appetite. The owner reported seizure-like episodes involving falling over, crying, leg stretching, and then slowly recovering. The episodes lasted approximately 30 seconds with full recovery within a few minutes. The first episode was three months prior. The patient had one episode the previous week and four episodes this week.
CBC/Chemistry- WNL
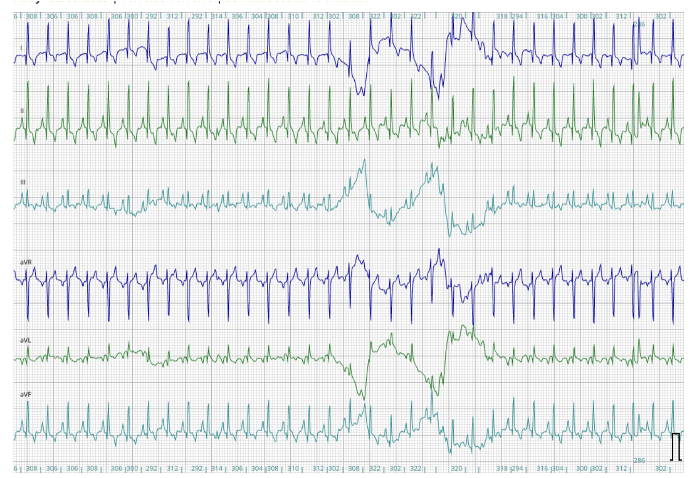
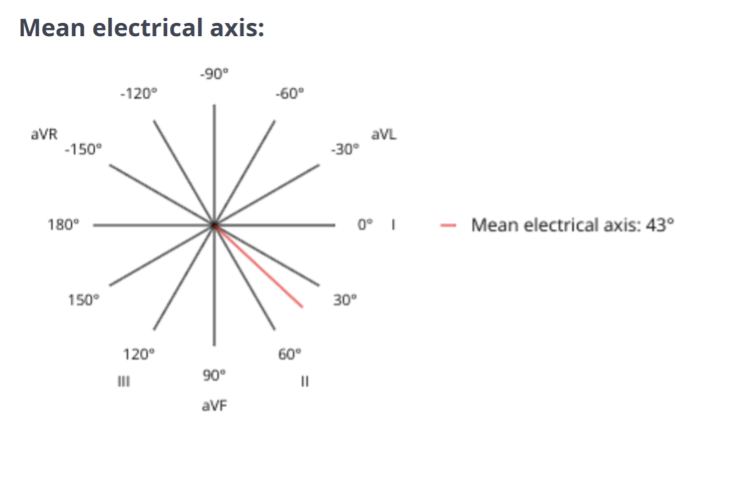
A 6-lead ECG is available at 25mm/s; 10mm/mV. The average heart rate is 180bpm with a regular rhythm. The rhythm is sinus in origin, with a P for every QRS complex and vice versa. The P wave morphology is positive with a normal dimension. Normal PR. The QRS morphology is positive with normal dimension. Mean electrical axis (MEA) is normal. No ectopic beats, pauses, or dysrhythmias observed. ECG diagnosis: Normal sinus tachycardia.
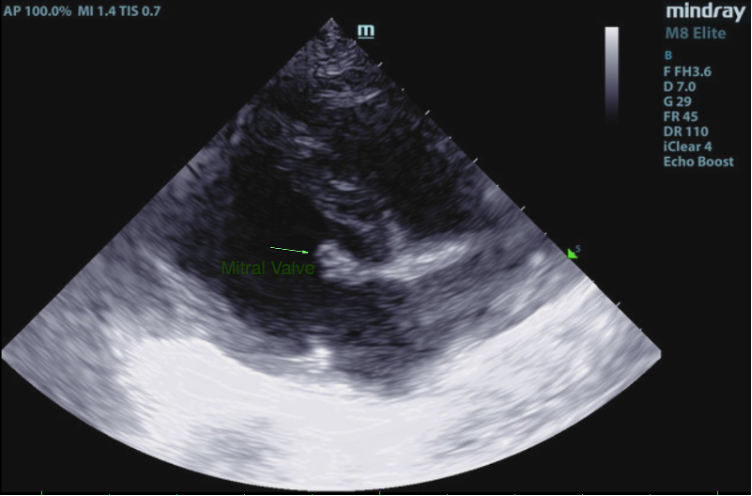
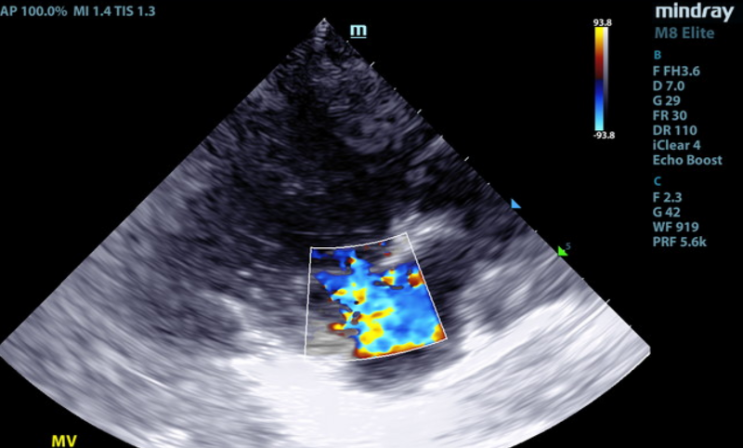
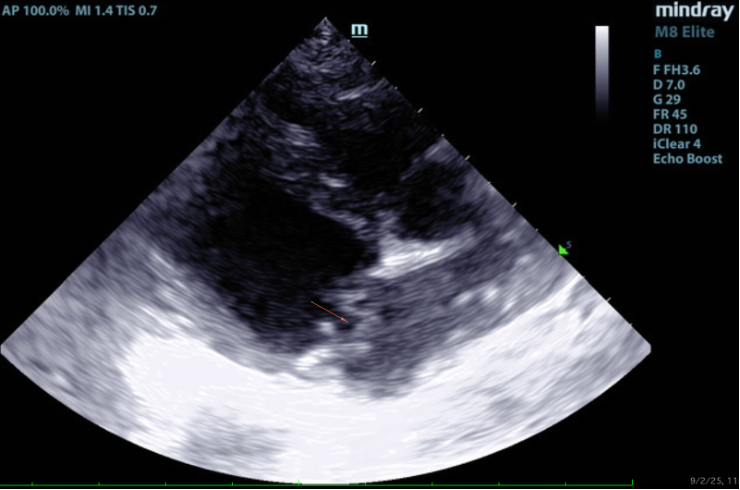
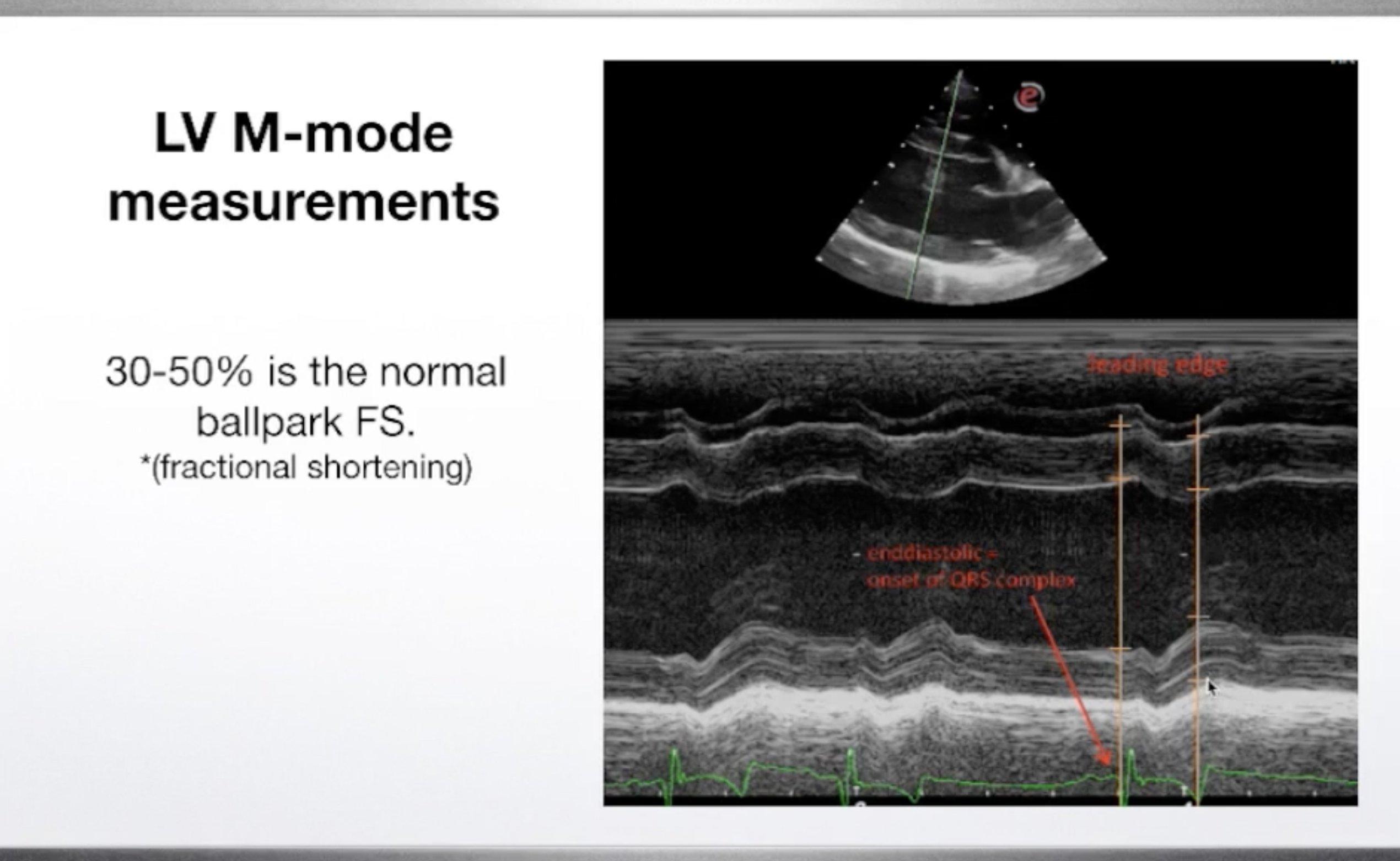
2D, M-mode, color flow, and Doppler imaging is available. The mitral valve is diffusely thickened with prolapse into the left atrial lumen. There is moderate eccentric mitral regurgitation present.
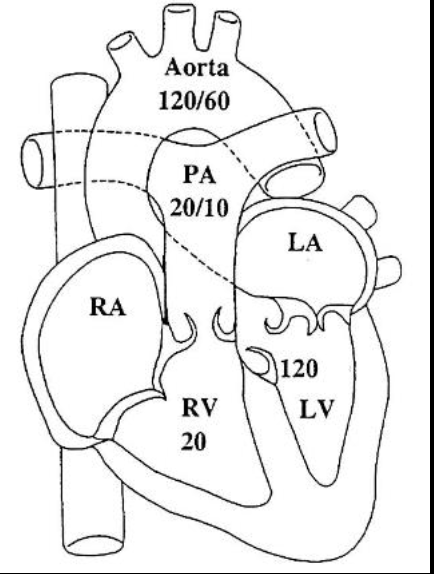
There is moderate left atrial enlargement. There is mild left ventricular dilation. Left ventricular systolic function is adequate. There is normal systolic flow velocity across the aortic valve; no insufficiency. The aortic valve appears normal. Mild right atrial/ventricular enlargement. The tricuspid valve is mildly thickened with moderate tricuspid regurgitation. The tricuspid regurgitant velocity is consistent with moderate to severe pulmonary hypertension (PH). The pulmonary artery is prominent. Normal aortic and pulmonic outflow velocities. No aortic insufficiency (AI) or pulmonary insufficiency (PI). No pericardial/pleural effusion or cardiac masses are seen.
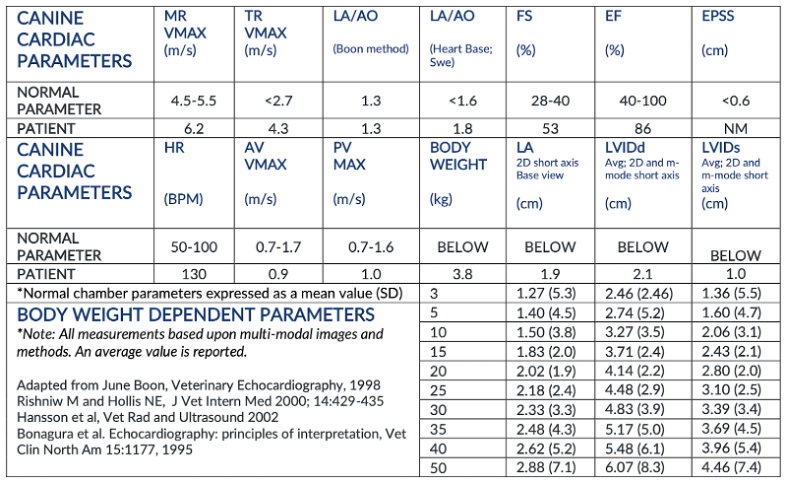
In this patient there is moderate left atrial enlargement, mild left ventricular enlargement, and mild right atrial and ventricular enlargement.
Chronic degenerative valve disease is causing moderate mitral and tricuspid regurgitation.
Moderate left atrial enlargement indicates there may be elevated risk for spontaneous congestive heart failure in the future. Moderate pulmonary hypertension is also identified with right heart and main pulmonary artery (MPA) enlargement. Given the combination of findings, pimobendan and sildenafil are recommended at this time in this patient at dosages indicated in the plan below. The ECG is unremarkable with a normal sinus tachycardia.
Assuming the episodes are exertional in origin, these may certainly be related to the finding of pulmonary hypertension. If this does not describe their genesis, a primary neurologic episode would be more likely. Pulmonary arterial hypertension (PAH) is often secondary to chronic respiratory disease; however, no chronic symptoms are noted in the history, and the cause remains open.
Determine if episodes are exertional in nature or random.
Chronic degenerative valve disease and moderate pulmonary hypertension. If episodes are exertional in origin then pulmonary arterial hypertension is suspected to be the cause.
A 6-lead ECG allows the cardiologist to evaluate the electrical impulses of the heart from different degrees around the electrical axis of the heart. In general, veterinary professionals are accustomed to evaluating lead 2.
Pulmonary hypertension is a sustained elevation in mean pulmonary arterial pressure > 25 mmHg or echocardiogenic estimated pulmonary arterial pressure > 30 mmHg. Normal mean pulmonary arterial pressure is 10–15 mmHg.
Dogs with PH are usually classified under 6 groups:
1. Pulmonary arterial hypertension
2. Left heart disease
3. Respiratory disease/hypoxia
4. Pulmonary thromboemboli
5. Parasitic disease (Dirofilaria and Angiostrongylus)
6. Multifactorial or unclear mechanisms
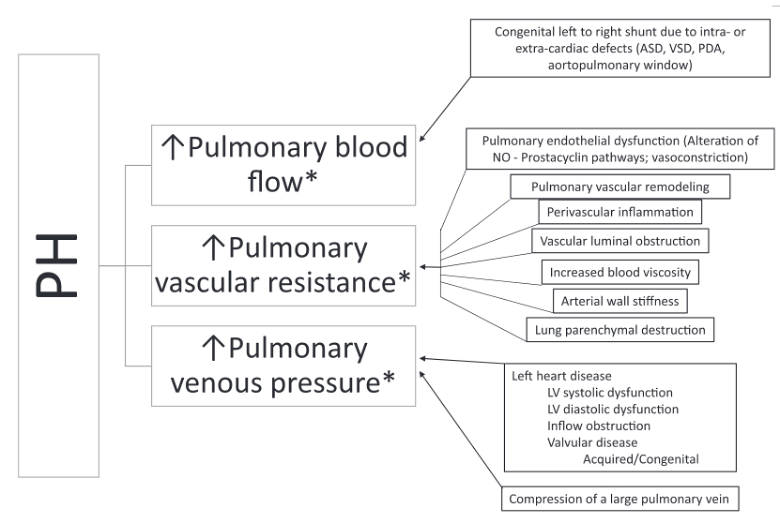
Image from the ACVIM Consensus statement on PH summarizing the pathophysiology creating PH.
The standard method for diagnosis of PH is direct assessment of pulmonary arterial pressure (PAP) by right heart catheterization (RHC). RHC is rarely used for definitive diagnosis in dogs and echocardiography is used to look for cardiac changes that occur secondary to PH and to estimate PAP using Doppler tracings of tricuspid regurgitation. Clinical presentation and echocardiography are the most common methods used to diagnose PH.
The modified Bernoulli equation converts Doppler velocity to pressure using the following equation:
PG = 4(V2)^2 (
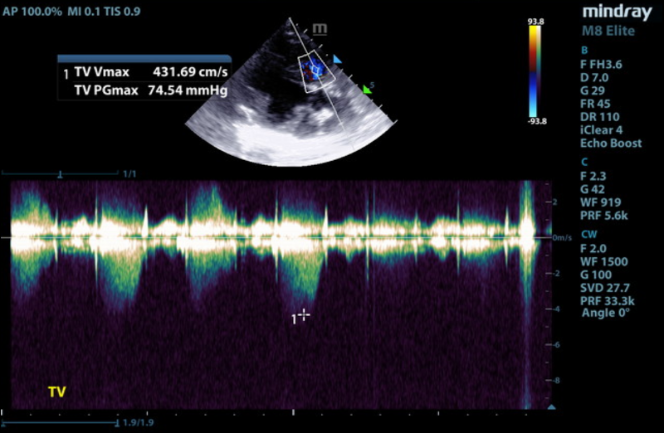
Doppler imaging is the best noninvasive test to diagnose PH. Peak tricuspid regurgitation (TR) velocity and gradient can estimate peak systolic right ventricular pressure. Assuming pulmonic stenosis is not present, TR velocity also correlates with systolic pulmonary arterial pressure. It can be used to classify PH as follows:
1) Mild: 2.8–3.5 m/s, PG 31.4–50 mmHg
2) Moderate: 3.5–4.3 m/s, PG 50–75 mmHg
3) Severe: > 4.3 m/s, PG > 75 mmHg
In this case, the TR Vmax (peak tricuspid regurgitation velocity) was measured at 4.3 m/s on CW Doppler. Plugging this value into the modified Bernoulli equation gives an estimated peak systolic right ventricular (RV) pressure of 74 mmHg. There was no pulmonic stenosis present so peak systolic RV pressure is equal to peak systolic pulmonary arterial pressure of 74 mmHg, moderate to severe pulmonary arterial hypertension.
Treatment of PH is aimed at decreasing the risk of progression of PH and treating underlying diseases contributing to PH. Please see the ACVIM consensus statement on recommended treatments based on classification of PH.
Institute heart muscle support: pimobendan 0.25–0.3 mg/kg PO BID. Institute sildenafil 1–2 mg/kg PO Q8h. Further work up for the episodes as discussed if non-exertional in origin.
Recommend monitor for progression with a recheck echocardiogram in 6 months, sooner if any development of clinical signs. Omega fatty acid supplementation and mild salt restriction may also be of some long-term benefit. Monitor for development of a progressive cough, labored breathing, exercise intolerance or collapse episodes.
Elective anesthesia is not advised.
“It is key to correctly identify the exact anatomic features of the stenosis.
In cases of valvular stenosis, the diameter of the pulmonary annulus in comparison with the aortic annulus helps to identify hypoplasia.”
The Curbside Guide, Page 438
Let us show you how to easily acquire great diagnostic imaging sets!
Your reference guide for echo images: Learn what normal looks like so that you can more readily identify abnormal. This 90+ video & image library contains normal & age-related presentations in dogs & cats and serves as an excellent reference for both beginners and experienced sonographers.
($24.99)
Join SonoPath’s founder and CEO Dr. Eric Lindquist as he guides you through SonoPath’s 7-manuever, 4-point Echo progression. Appropriate for all levels of sonographer, this pre-recorded online course allows you to learn at your own pace, review material as you need, and provides all you need to progress your echo image sets!
(NOTE: This course includes the 7-point Echo Progression lecture)
6 RACE-approved CE credits
$799.99 (normally $999.99) for the month of March only!

Your first step to a complete Echo image set. The SDEP® Echo progression utilizes a numbered protocol to optimize every region of the heart to evaluate functions, velocities, pressures and chamber sizes.
2 RACE-approved CE credits ($189.99)
References
1. Reinero C, Visser LC, Kellihan HB, et al. ACVIM consensus statement guidelines for the diagnosis, classification, treatment, and monitoring of pulmonary hypertension in dogs. Journal of Veterinary Internal Medicine 2020;34:549–573.
2. Boon JA. Veterinary echocardiography. 2nd ed. Ames, Iowa: Wiley-Blackwell; 2011.