Right Divisional Intrahepatic Portosystemic Shunt In An 8-Week-Old Intact Male Golden Retriever: Our Case Of the Month September 2023

What do you do when your Rocket malfunctions?
Karen Ebersole, DVM, DABVP, owner of Scanvet, which provides high-level ultrasound services in central Maine, from Portland to Augusta and SonoPath specialist, found a suspect liver shunt in an 8-week-old Golden Retriever named Rocket. Dr. Ebersole, along with her fluffy co-pilot Rocket, took a trip to the SonoPath Imaging Center for further interrogation of the liver shunt. Sebastian Schaub, DVM, Dr. med. vet., Dipl. ECVDI (Radiology) and SonoPath specialist, interpreted Rocket’s CT study.
History
Rocket was initially presented for seizures at four weeks old. Physical examination found seizure activity, neurologic changes, and a low grade heart murmur. CBC and blood chemistry revealed anemia, low protein and an elevated ammonia level. Suspect right divisional intrahepatic shunt based on ultrasound. Current Meds: Lactulose 1ml bid; Amoxicillin (250mg/ml) 0.6ml bid; Gabapentin 100mg 8:30am today; L/D diet. 8/2/2023-Bile Acids Pre 40.7; Post 53.7; 7/31/2023-BUN 6; Na 141; TP 3.6; Albumin 1.4; Globulin 2.2; ALP 414; Ammonia 141; RBC 3.36; HCT 21.3; HGB 7.3
Patient information
Age: 8-week-old
Gender: Intact male
Species: Canine
Breed: Golden Retriever
CBC/Chem: RBC 3.36, HCT 21.3, HGB 7.3, BUN 6, Na 141, T.P. 3.6, Albumin 1.4, Globulin 2.2, ALP 414, Ammonia 141. Bile Acids Pre: 40.7, Post: 53.7.
Ultrasound image interpretation
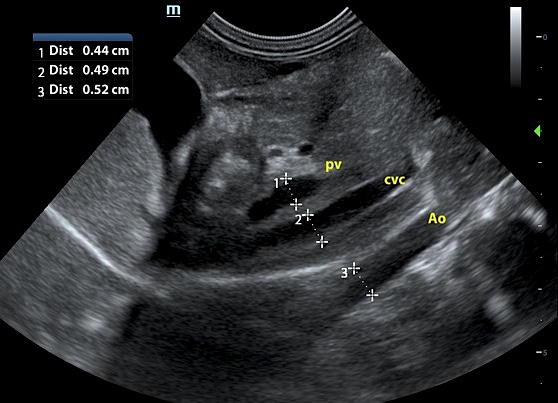
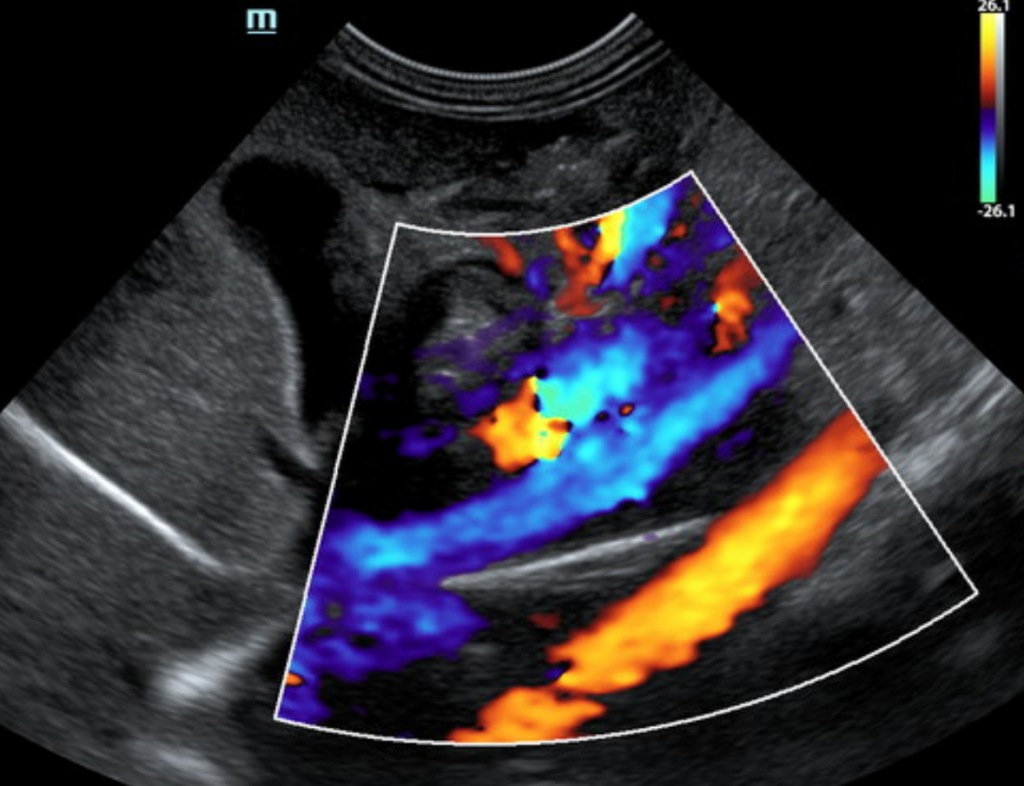
Liver: The liver was subjectively subnormal in size with atrophy of the right liver lobes. The capsule contour was smooth. There was subjectively decreased vascularity in the liver. The PV:CVC:AO ratio is a normal 1:1:1 in the extra-hepatic region, ruling out a EHPSS. On examination of the intra-hepatic branching of the portal vein, the central and left divisional branches appear normal, and thus can be ruled out as a cause of intrahepatic shunting. However, the right divisional branch of the portal vein lacks the normal narrowing/branching shape and may be connecting with the vena cava. This consists of a short connection at the level of the diaphragm. This would need to be evaluated and potentially confirmed with CT with contrast.
Kidneys: Both kidneys were mildly swollen in contour and potentially increased in size. The capsule contour was smooth with no deviation. The internal architecture was normal. There was no pelvic dilation. The left kidney measured 5 in length. The right kidney measured 5.5 cm in length.
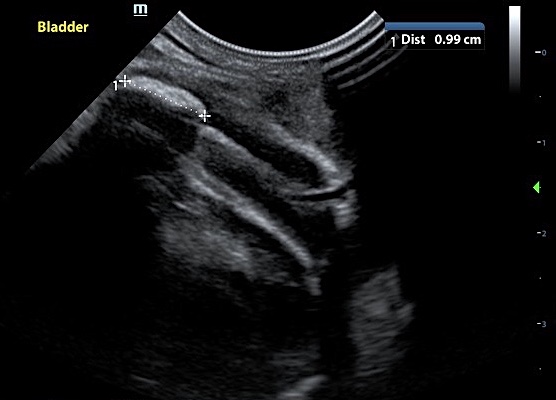
Bladder: The bladder contained minimal amounts of urine, primarily anechoic with mild echogenic suspended sediment. There was a 1 cm strongly shadowing hyperechoic density in the bladder. There may be a second area of strongly shadowing sediment towards the trigone/urethra.
Ultrasound diagnosis
Liver: Suspected right divisional intra-hepatic portosystemic shunt (IHPSS) Subjectively subnormal liver size, particularly the right liver.
Kidney: Bilateral renomegaly – suspect swelling secondary to IHPSS.
Bladder: Bladder stone/s or conglomeration of mineralized sand.
CT image interpretation
Liver: The portal vein presents a normal order of its tributary veins. Originating from the right lateral intrahepatic branch of the portal vein, a short anomalous connection is seen, draining into a right hepatic vein. The anomalous vascular connection is measuring 6.8 mm in diameter.
Kidneys: Both kidneys present an increased volume. After contrast administration a bilaterally symmetric and uniform nephro- and pyelogram is noted.
CT diagnosis
Liver: Right divisional intrahepatic portosystemic shunt.
Kidneys: Renomegaly.

Case status 8/25/2023
The findings from the CT study are consistent with a congenital single intrahepatic portosystemic shunt originating from the right lateral intrahepatic branch of the portal vein, presenting as a short anomalous vascular connection. Hepatic encephalopathy is a potential cause for the neurological clinical signs. Slow progressive closure technique (coil, ameroid) is the therapy of choice. Empirical treatment until functional shunt closure along with feeding of a hepatic diet is recommended.
Case update: 12/20/2023
Rocket is doing very well with medical and diet management. He is scheduled to go to Tufts on March 15th for his consult for coil placement. Tufts wanted him to get to 8-9 months of age to be able to choose an appropriate size coil for best success. He will likely have a follow-up CT and serial blood chemistry checks following his coil placement procedure. See Rocket’s full journey by clicking HERE.
