
A 10-year-old FS hound mix presented to Wellesley Animal Hospital for dental disease and to have a dental prophy performed. On physical examination, Dr. Ryan Leal noted a grade III-IV/VI left-sided murmur and recommended an echocardiogram. At that time the owner elected to work up the murmur prior to anesthesia being performed for the dentistry.
Thank you Ryan Leal, DVM at Wellesley Animal Hospital for your thorough and skillful SDEP® diagnostic cardiac image set and case management, and thank you Eric Lindquist DMV, DABVP, Cert. IVUSS, for your comprehensive interpretative report.

Abnormal PE/Chem/CBC/UA Results:
PE: grade 3-4/6 left-sided heart murmur; heavy dental calculus and gingival epulis on 103/104 and 203/204 CBC: WNL Chem: WNL ProBNP: 3988 (H) T4: WNL

ULTRASONOGRAPHIC EXAMINATION OF THE HEART
The echocardiogram in this patient demonstrated enlarged left atrial size. Chamber volumes and echogenicity were normal. The cranial and caudal mitral valve leaflets presented normal linear structure, extension in systole, and union in diastole. No significant dystrophic or vegetative changes were noted. The left ventricle demonstrated excessive volume (LVIDd measurement below). Ventricular function was subnormal expressed by the fractional shortening (FS) measurement. Myocardium appeared subjectively thin typical of DCM. The left ventricular outflow tract demonstrated normal laminar flow and subjective structural integrity. The right atrium and auricle revealed normal size, structure and content. No evidence of masses or chamber overload. Tricuspid valvular assessment demonstrated adequate linear morphology. The right ventricle was of normal size (1/3 diameter of LV), chordae structure, myocardial echogenicity and thickness. Pulmonic tract assessment revealed normal valve structure, laminar flow, and diameter (approx.1:1 PA/AO ratio). No visible pericardial or free pleura fluid was noted. The cranial mediastinum and pericardial regions were free of masses in the visible window. Arrhythmogenic activity was noted. The hepatic veins were not dilated.




ULTRASONOGRAPHIC FINDINGS
DCM presentation. Myocarditis and nutritional cardiomyopathy possible.
INTERPRETATION OF THE FINDINGS & FURTHER RECOMMENDATIONS
Quadrotherapy is recommended with pimobendan at 0.3 mg/kg b.i.d., ace inhibitor at 0.5 mg/kg s.i.d. progressing to b.i.d., spironolactone at 1-2 mg/kg b.i.d. Thyroid assessment is warranted as well as baseline cortisol to ensure that hypothyroidism and Addison’s are not playing a role. EKG (due to the arrhythmogenic activty ) and blood pressure measurements are indicated as well as taurine levels. If any history of infectious disease such as Lyme or Bartonella have been in play then a secondary myocarditis should be considered. A recheck echocardiogram is recommended in a month. If any pulmonary edema is present then Lasix can be added to the protocol. Taurine supplementation would be appropriate. If any infectious agents are suspected in this patient then enrofloxacin and clindamycin combination can be considered to treat underlying myocarditis.
Patient Outcome:
One year post-diagnosis, the patient is reported to be doing well. She was started on spironolactone (25mg PO BID), enalapril (10mg PO BID), pimobendan (5mg PO BID), and Cardiac Care diet by Purina. She is given K9 Advantix and Sentinel for preventatives. Unfortunately she still has dental disease (which was the reason the echo was performed – working up the murmur prior to a dentistry) and a follow-up echocardiogram is recommended.
General Discussion of DCM
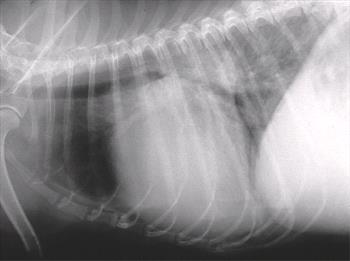

Example radiographs of a DCM patient
Dilated cardiomyopathy is a disease of the myocardium that causes decreased contractility and a secondary, compensatory ventricular dilation. Causation can be attributed to primary sources such as genetic, idiopathic, and inflammatory, while secondary factors can be from medications (doxorubicin), infections, metabolic, and nutritional causes. Clinical signs of DCM vary based on the amount of dilation (eccentric hypertrophy). Generally systolic dysfunction leads to a decreased stroke volume which causes activation of the renin-angiotensin-aldosterone system (RAAS) and fluid retention which increases preload to restore stroke volume. However, myocardial failure continues and eventually the increased preload leads to increased end-diastolic pressures and congestive heart failure (CHF). As eccentric hypertrophy continues, electrical instability across the myocardium may lead to arrhythmias. A heart murmur of mitral or tricuspid regurgitation, as well as an irregular rhythm, may be auscultated. Atrial fibrillation is one of the most common arrhythmias detected. Ventricular premature complexes may also be seen.
As a primary disease, DCM is found to be an inherited trait in several breeds including the Portugese Water Dog, Irish Wolfhound, Great Dane, Newfoundland, Standard and Giant Schnauzer, Doberman Pinscher, Welsh Springer Spaniel, and Boxer (arrhythmogenic right ventricular cardiomyopathy is more common). Mode of inheritance varies by breed from autosomal dominant in the Doberman Pinscher to an autosomal recessive trait in the Portugese Water Dog. Genetic testing is available for each breed.
Myocarditis can cause a type of secondary DCM in which the myocardium (middle layer of cardiac muscle) becomes inflamed. It can develop into inflammatory cardiomyopathy – a state where chronic inflammation causes cardiac dysfunction and ventricular remodeling. Often, there are no symptoms with myocarditis until the severity leads to heart failure, at which time the patient may suffer weakness, dyspnea, coughing, and arrhythmia among other signs. An example is Chagas myocarditis from the protozoal parasite Trypanosoma cruzi. Other causes of myocarditis can be viral, inflammatory, and immune mediated.
Other causes of secondary DCM include nutritional. In Golden Retrievers and Cocker Spaniels, this may be attributed to taurine deficiency. In other dogs it has been associated with diets that are grain free and high in legumes and peas. In some cases, clinical signs may be able to be reversed with supplementation of taurine.
Finally, causes such as doxorubicin toxicity, hypothyroidism, and tachycardia-induced can lead to a secondary DCM.
References:
Saunders, A. Myocarditis in Dogs and Cats. Southwest Veterinary Symposium. College Station TX 2012.
O’Grady, M., O’Sullivan, M,L. Pathophysiology of Dilated Cardiomyopathy. Am College Vet Internal Med Forum : ACVIM 2012.
Galles, B, Lake-Bakaar, G. Cardiomyopathy, Dilated (Canine). VINcylclopedia of Diseases Jan 2023.
Looking to enhance the range of your ultrasound diagnostic efficiency?
