
rDVM and sonographer: Katelyn Mazzochette, DVM, Airpark Animal Hospital
SonoPath Specialist: Eric Lindquist, DMV, DABVP, Cert IVUSS
Worked cooperatively with Internist and Surgeon for further diagnostics (CT scan, metanephrine test) and adrenalectomy.

The patient presented to her veterinarian for a one-week history of vomiting, diarrhea, increased panting, decreased appetite, and lethargy. On physical exam she was alert and responsive but subdued compared to her normal energy level. She had mild abdominal discomfort and was panting. She has a history of chronic, intermittent, gastrointestinal disease that has previously been managed well on I/D diet. The rDVM was concerned about an acute flare up of her GI disease, possible inflammatory bowel disease, dietary indiscretion, infectious, and/or hemorrhagic gastroenteritis and occult neoplasia.
CBC
Neutrophils 12.5 K/uL (2.95–11.64) HIGH
ACTH Stim
WNL
Texas A&M GI Panel
Cobalamin 168 ng/L (251–908) LOW
Interpretation: Consistent with distal small intestinal disease, EPI, or small intestinal bacterial overgrowth.
Radiographs
Lungs and heart normal, significant gas noted in colon and stomach, no foreign body identified.
SDEP® Position 5.
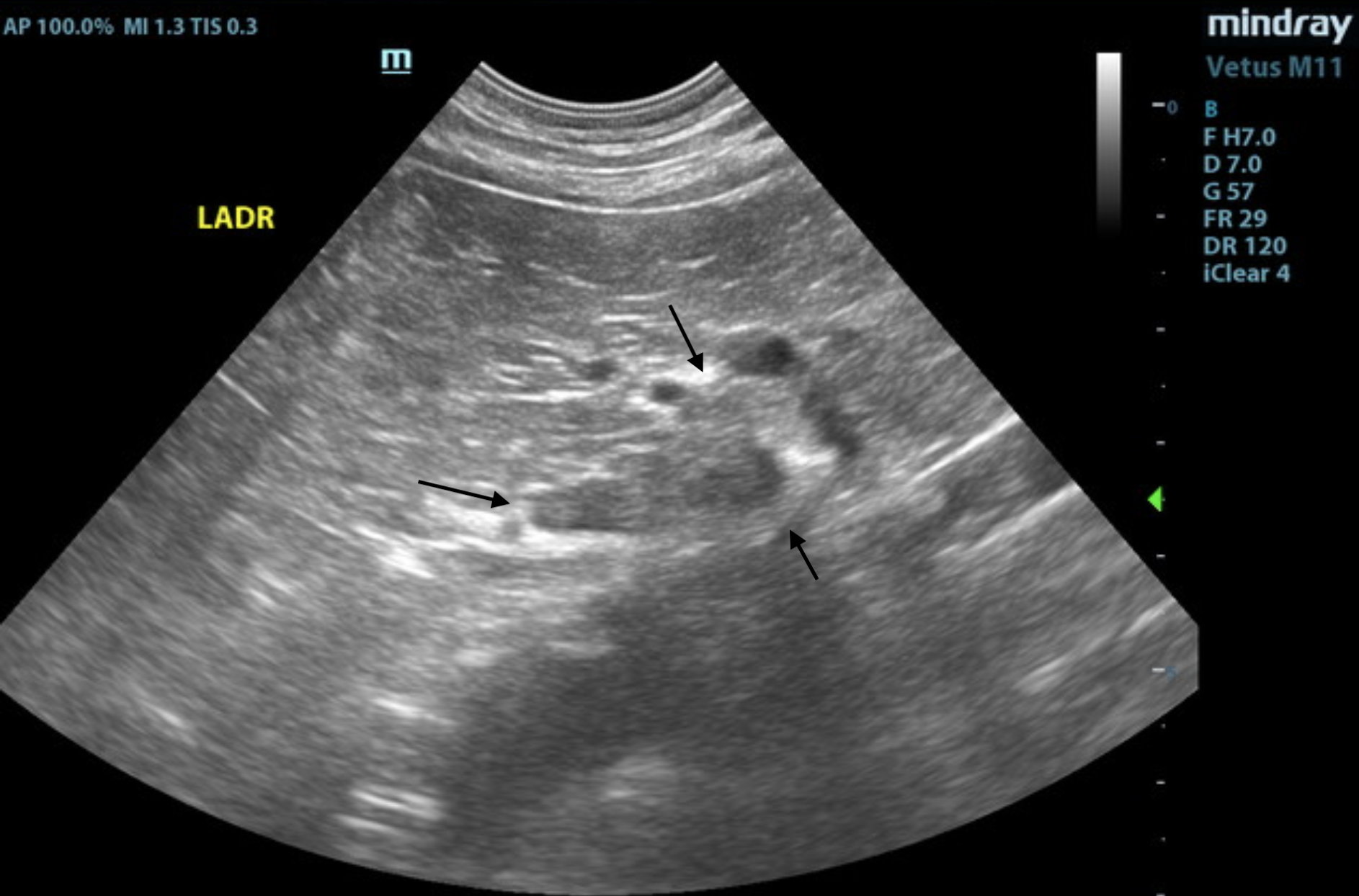
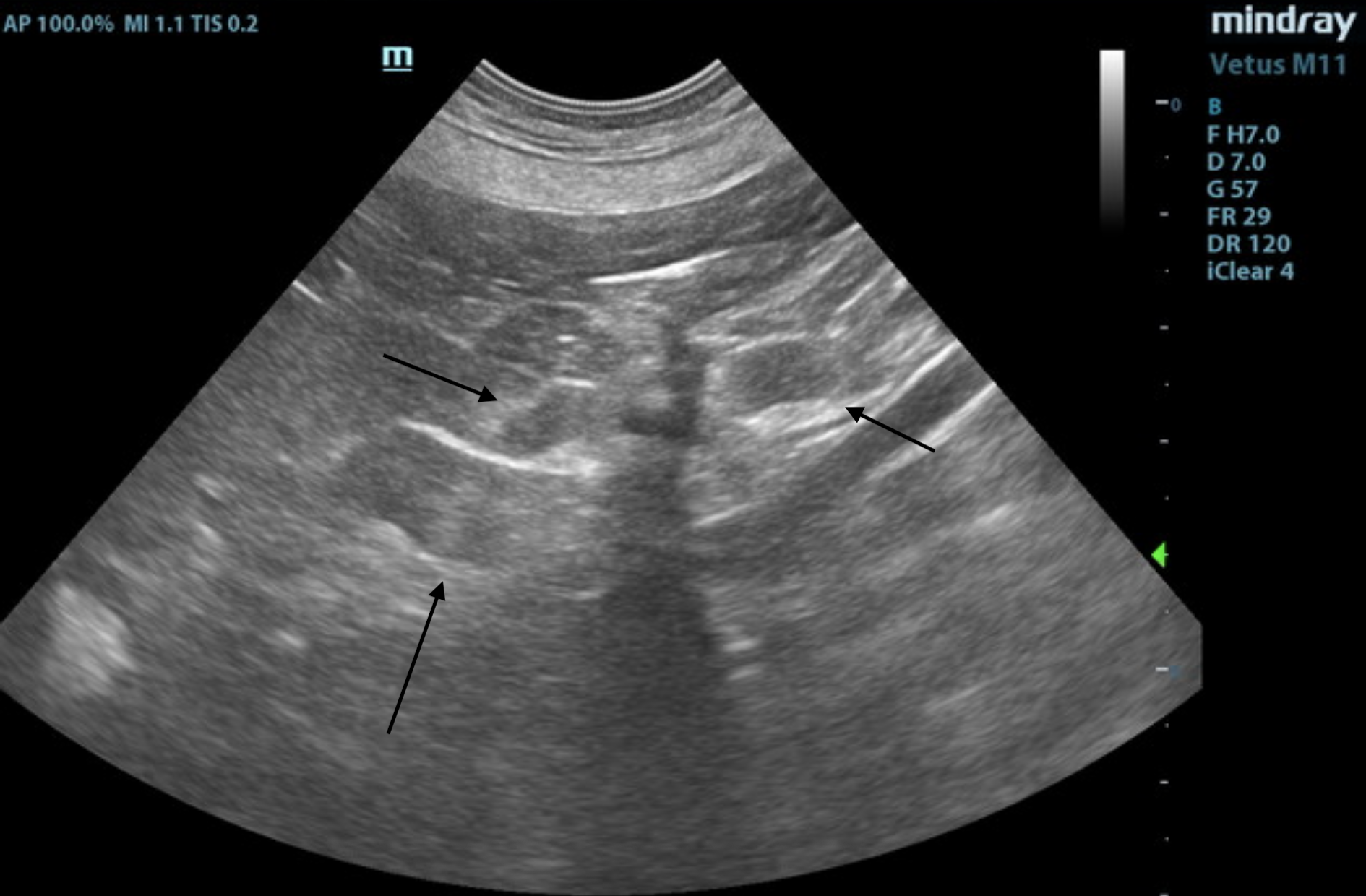
Video 1. Video of the left adrenal gland showing the enlarged, irregular caudal pole.
SDEP® Position 5.
Video 2. Video showing an enlarged spleen with some irregular nodular changes. SDEP® Position 7.
Video 3. Video showing the mild GI thickening. SDEP® Position 15.
Urinary System
The urinary bladder, trigone, and pelvic urethra presented normal thicknesses and normal tone. The ureters were not visible which is normal. No uroliths or sediment were visualized and anechoic urine was present. No evidence of inflammatory or neoplastic changes were noted. Ureteral papillae were normal. The pelvic urethra was imaged 2.0 cm beyond the cystourethral junction.
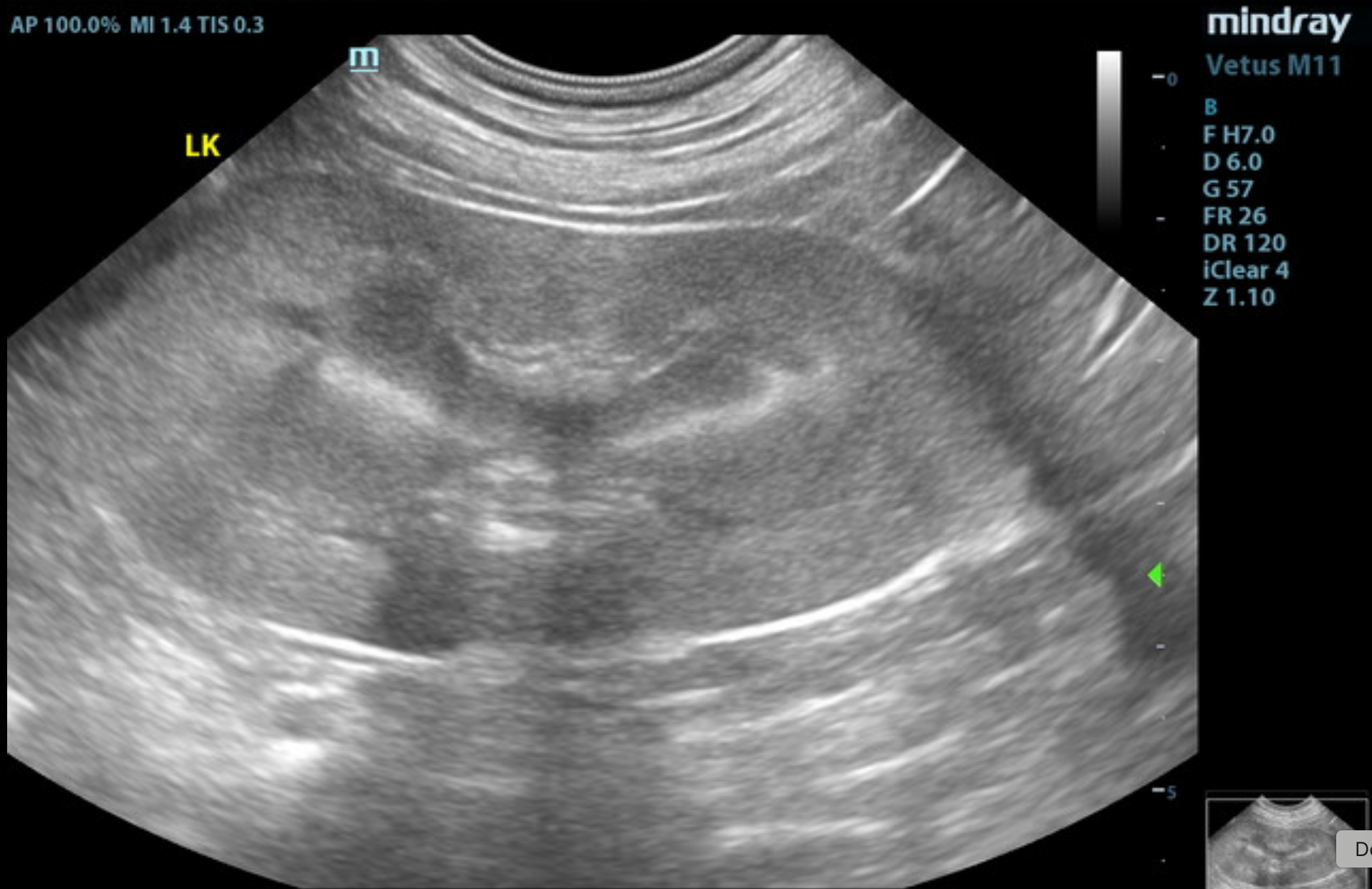
The kidneys revealed largely normal size and structure. Corticomedullary definition and ratio (cortex 1/3 of medulla) were essentially maintained with some age-related loss of curvilinear patterns regarding the capsule and C/M junction. The cortices presented largely uniform texture with some increased echogenicity expected for this age patient. Medullary structure differed distinctly from that of the cortex and no evidence of pelvic dilation was present. The right kidney measured 5.6 cm. The left kidney measured 6.6 cm.
Adrenal Glands
The left adrenal gland was enlarged at the caudal pole, measuring 0.93 cm at the caudal pole and 0.46 cm at the cranial pole and 2.25 cm in length. It was irregular in contour with capsular expansion. Minor heterogeneity noted at the phrenic vein, consistent with phrenic occupation. Mineralization was also noted.
The right adrenal gland was normal in size, measuring 2.9 cm x 0.78 cm at the cranial pole and 0.59 cm at the caudal pole.
Spleen
The spleen was enlarged with irregular nodular changes.
Liver
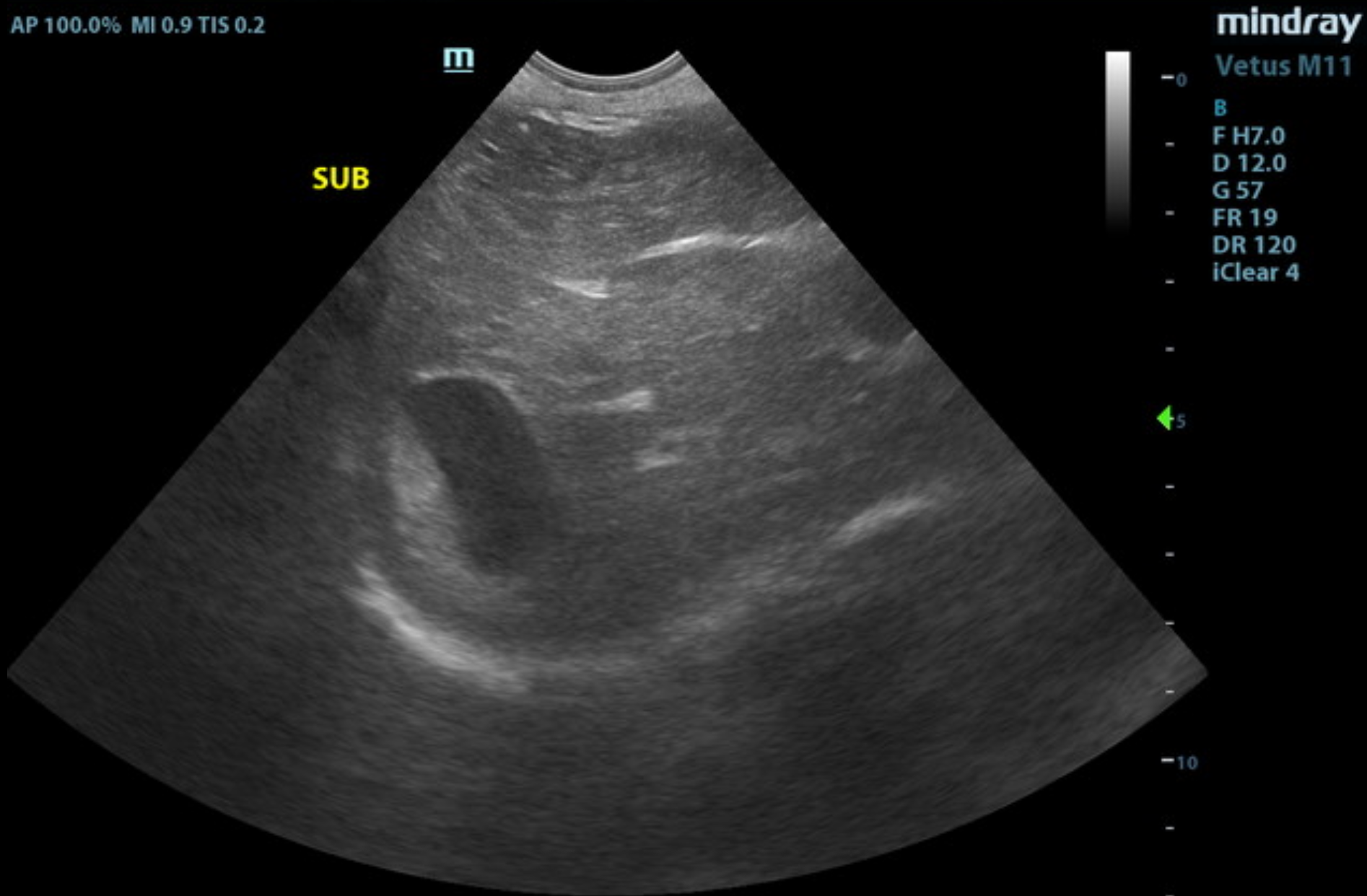
The liver images from right and left intercostal as well as subcostal views revealed subjectively normal liver size, contour, and structure. Some age-related parenchymal remodeling was noted but likely not clinically significant at this time. Vascular and biliary tracts were of normal volume, and no evidence of congestion was noted. The gallbladder presented some dependent debris with essentially normal contour. The cystic and common bile ducts were normal. No overt evidence of active inflammatory, infiltrative, or regenerative pathology was noted but should be paired with current or past LE elevations regarding any clinical significance to this presentation. The hepatic lymph nodes were unremarkable.
Gastrointestinal
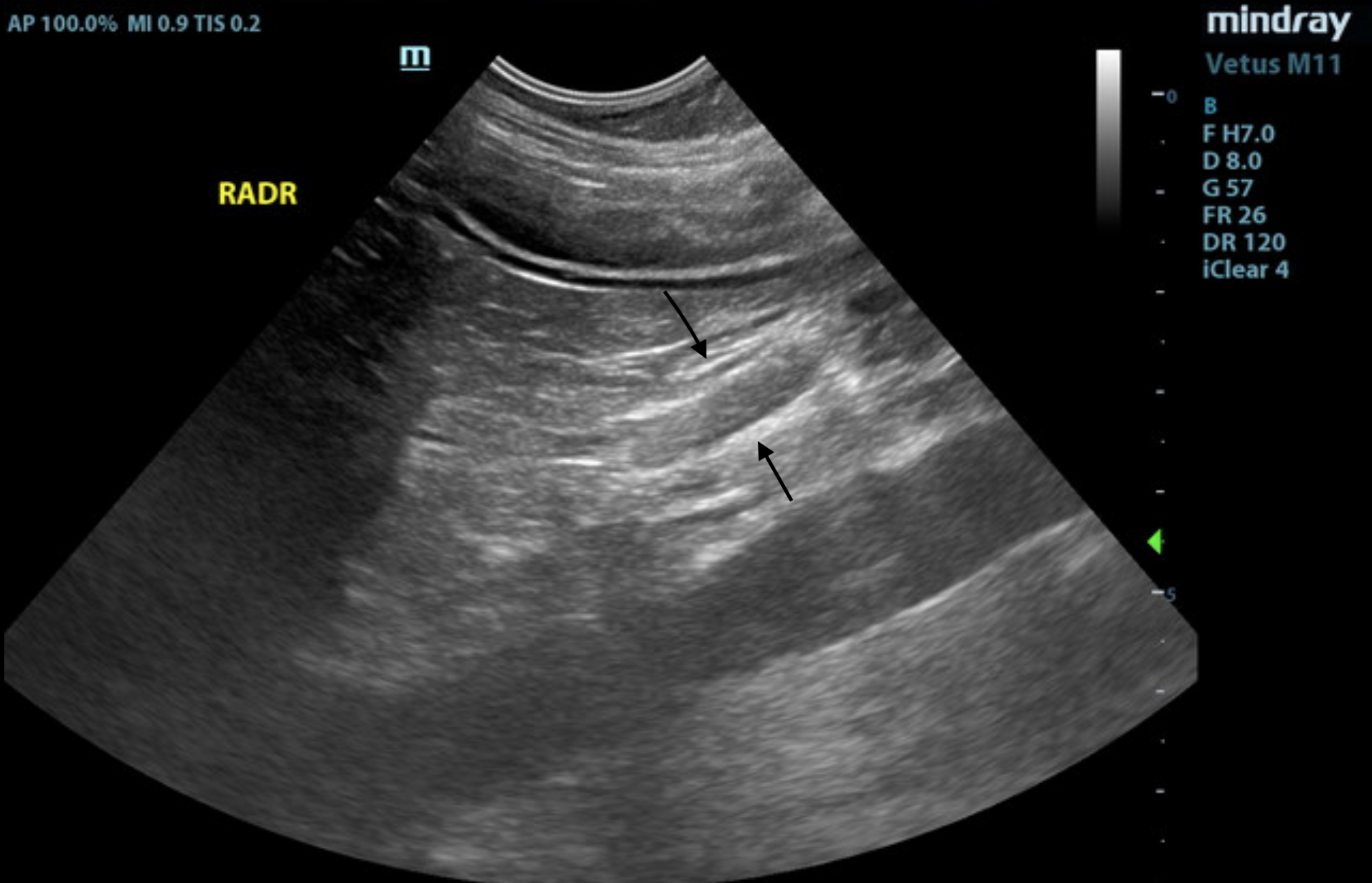
The gastrointestinal presentation revealed mild uniform prominence of the gastric mucosa as well as areas of “ropey” small intestinal wall with slight disruption of the normal 1:3 muscularis/mucosal ratio. The intestinal submucosa was slightly irregular, thickened, and hyperechoic, suggestive of low grade, chronic disease. No evidence of obstruction was present. Chronic inflammatory bowel disease is likely with a low possibility of an early neoplastic event such as lymphoma. Full thickness tissue biopsies via open laparotomy, ideally guided by intraoperative ultrasound in order to obtain the most representative mural sample, would be necessary to rule out this possibility.
Mesenteric lymph nodes were mildly enlarged, reactive.
Pancreas
The base and limbs of the pancreas were observed to be largely isoechoic to surrounding omental fat. Pancreatic duct and capsular contour were acceptably normal and parenchyma respected normal curvilinear patterns. No overt evidence of active inflammatory or neoplastic disease was noted.
• Irregular left adrenal gland — either thrombosis or potential emerging neoplasia
• Mild, chronic GI thickening and reactive mesenteric lymph nodes
• Hepatic remodeling
• Splenic enlargement
• Age-related renal changes
FNA of the spleen and liver could be justified in this patient. There is concern about potential emerging carcinoma or pheochromocytoma of the left adrenal.
Serial blood pressure measurements are recommended in this patient. If hypertension is an issue, metanephrine level is recommended. If the patient appears Cushingoid and urine specific gravity is less than 1.020, then work-up for adrenal-dependent Cushing’s is indicated. Recheck is recommended in 2–3 weeks to assess for any progression of the adrenal gland. If surgery is to be performed to remove the left adrenal gland, full thickness GI biopsies indicated.
The adrenal gland is composed of an outer cortex and inner medulla. The adrenal cortex contains three layers, each producing a specific hormone. In the cortex, the outermost layer is the glomerulosa which produces aldosterone, the middle fasciculata produces cortisol, and the inner reticularis layer produces androgens. The medulla produces catecholamines.
Adrenocortical carcinomas are the most common adrenal tumor found in dogs followed by pheochromocytomas (medulla), metastatic lesions, and adenomas. Cortical hyperplasia is also a very common finding for enlarged adrenal glands.
Dogs with adrenal tumors are usually middle-aged or older and present with signs such as polyuria, polydipsia, polyphagia, panting, weakness, lethargy, anxiety, restlessness, and a potbellied appearance. Adenomas are usually incidental findings on an ultrasound scan and not usually associated with clinical signs.
Ultrasound is useful for identifying lesions in the adrenal glands. Unilateral lesions > 20 mm with vascular invasion have a higher chance of malignancy, while nodular bilateral lesions are more commonly associated with cortical hyperplasia.
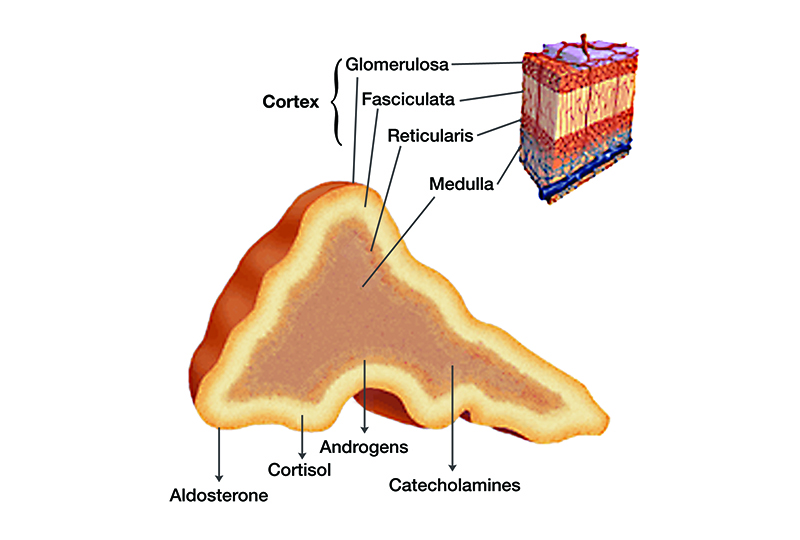
Image showing the functional layers of the adrenal gland and what hormones they produce. 1
As not all patients are able to have a CT performed or as an adjunct for completeness, it is valuable to include imaging of the “left adrenal from the right side” whenever an abnormality is noted from SDEP® Position 5 as part of the abdominal image set. This additional view can be considered a modification of SDEP® Position 14A and will capture phrenic invasion into the CVC.
From the right adrenal, follow the vena cava caudally and look for phrenic invasion
Angle between the CVC and the aorta to identify the left adrenal cranial to the left renal artery. Try to connect the phrenic vessels into the CVC
Color added
–
If an adrenal tumor is found then an ACTH stimulation test or LDDST, metanephrine urine test, and blood pressure can be performed to determine if the tumor is functional and cortisol or catecholamine secreting. These tests are not definitive as hormones can be secreted randomly.
Adrenalectomy is the treatment of choice for suspected malignant functional adrenal tumors.Histopathology of the tumor is required for definitive diagnosis of tumor type. 2 3 4
The patient was referred to an internal medicine specialist for continued workup of her chronic GI issues and adrenal mass. A CT scan and metanephrine test were performed.
CT report
FINDINGS:
There is an ovoid hypoattenuating nodule within the caudal pole of the left adrenal gland measuring approximately 1.7 cm L x 1.1 cm H x 1.4 cm W. There is no definitive evidence of vascular invasion at this time. The liver shows normal attenuation and homogeneous contrast-enhancement. There are multifocal contrast-enhancing nodules throughout the spleen.
1. Left-sided adrenal gland nodule may represent benign (adenoma, nodular hyperplasia, myelolipoma) vs. malignancy (carcinoma, pheochromocytoma, others).
2. Splenic nodules may represent benign (ie. Nodular lymphoid hyperplasia, extra medullary hematopoiesis, others).
Metanephrine
WNL- Not definitive but less likely chance of pheochromocytoma
Surgery Report
An approximately 1.5x 2.0 x 1.5 cm bilobed, firm, left adrenal mass was observed. There was no
invasion into the aorta, vena cava, left phrenicoabdominal and left renal vasculature. A left adrenalectomy was performed and the patient recovered uneventfully.
Histopathology
Adrenocortical Carcinoma with neoplastic cells extending to the electrocauterized surgical margin.
Additionally in one section, the adrenal medulla has a nodular appearance, creating a vague mass effect. Unsure if this represents a pheochromocytoma or benign nodule.
Followup
Oncology recommended monitoring Angel for recurrence. This would include physical
exam, abdominal ultrasound every 3 months for the first year after surgery and then every 6 months.spa
“The larger the mass, the more likely metastasis has already occurred, despite a lack of detectable lesions on ultrasound and thoracic radiographs.
Invasion of the mass into surrounding organs or blood vessels also supports malignancy, as does the detection of additional mass lesions with abdominal ultrasound and thoracic radiographs.
Use of imaging modalities, such as CT and MRI, will likely provide additional data on the characteristics of specific adrenal lesions for use in diagnosis and treatment planning”
The Curbside Guide, Page 143
Section 3: Organ-Based Disease —Chapter 2: Adrenal Tumors
The 7 lessons include Anatomy and understanding, step-by-step instructions on image acquisition, as well as hand and probe positioning. Common challenges and practical solutions are covered. Lessons include a combination of still images, video clips, and downloadable Bootcamp audio files to help coach you to more efficient image acquisition.
($29.00)
SDEP® is a numbers-based, repeatable approach in a 17-point protocol that produces a full abdominal scan, from the deep pelvic urethra to diaphragm and everything in between. In this comprehensive series, Dr. Lindquist walks you through the needed probe movements on his patient with associated ultrasound images.
The bundle includes lecture and hands-on technique sections. This series is an excellent substitute when hands-on training is not possible, or as a supplement to hands-on learning after one of our SDEP® courses. The course is appropriate for ALL levels of scanning. Beginners can grasp, and build on the fundamentals.
Intermediate users can benefit by improving efficiency and image sets, while advanced users can push the paces on more advanced sonography techniques like shunt hunts, adrenals, and more.
6 RACE-approved CE credits
($999.99)

References
1. agraham. Canine Hypoadrenocorticism: Overview, Diagnosis, & Treatment. Today’s Veterinary Practice 2014. Available at: https://todaysveterinarypractice.com/endocrinology/canine-hypoadrenocorticism-overview-diagnosis-treatment/. Accessed March 2, 2026.
2. Philip R. Fox DVM. ACVIM 2015. VIN.com 2015. Available at: PHEOCHROMOCYTOMAS AND ADRENAL CARCINOMAS: DIAGNOSIS, SUPPORTIVE CARE, AND DEFINITIVE TREATMENT
3. Pagani E, Tarducci A, Borrelli A, et al. Accuracy of Ultrasonographic Measurements of Adrenal Glands in Dogs: Comparison with Necroscopic Findings. Anatomia, Histologia, Embryologia 2017;46:187–194.4. Pagani E, Tursi M, Lorenzi C, et al. Ultrasonographic features of adrenal gland lesions in dogs can aid in diagnosis. BMC Vet Res 2016;12:267.