
Referring DVM: Dr. Leanne Shutt at Animal Hospital of Boone
Sonographer: Dr. Kathleen Byrnes at Carolina Veterinary Mobile
Specialist (Radiology) Dr. Nele Eley (Ondreka), DipECVDI, at Sonopath
Surgical Referral: Dr. Chris Hoffman, DACVS at Western Carolina Veterinary Surgery

A six-year-old female spayed pit bull mix presented to her regular veterinarian for a one-week history of shaking, ADR, and crying out in pain. The patient has a history of bilateral medial luxating patellas and a partially torn CCL in her right hindlimb. The patient had a right TPLO and MPL stabilization surgery one year prior. Her current orthopedic exam was normal and no cranial drawer or thrust was elicited in the left hindlimb. She was treated for a suspected soft tissue injury with anti-inflammatories and rest. The patient continued to act very painful, continued crying out, and began holding her left hindlimb up occasionally. She became toe-touching lame in the left hindlimb. No cranial drawer, tibial thrust, or pain could be elicited on orthopedic exam. An orthopedic ultrasound of her left stifle was performed to determine if there was a partial injury to the left CCL or menisci.
CBC Hct 55.6% (30.3-52.3) High
Chem K+ 3.2 (3.5-5.8) Low
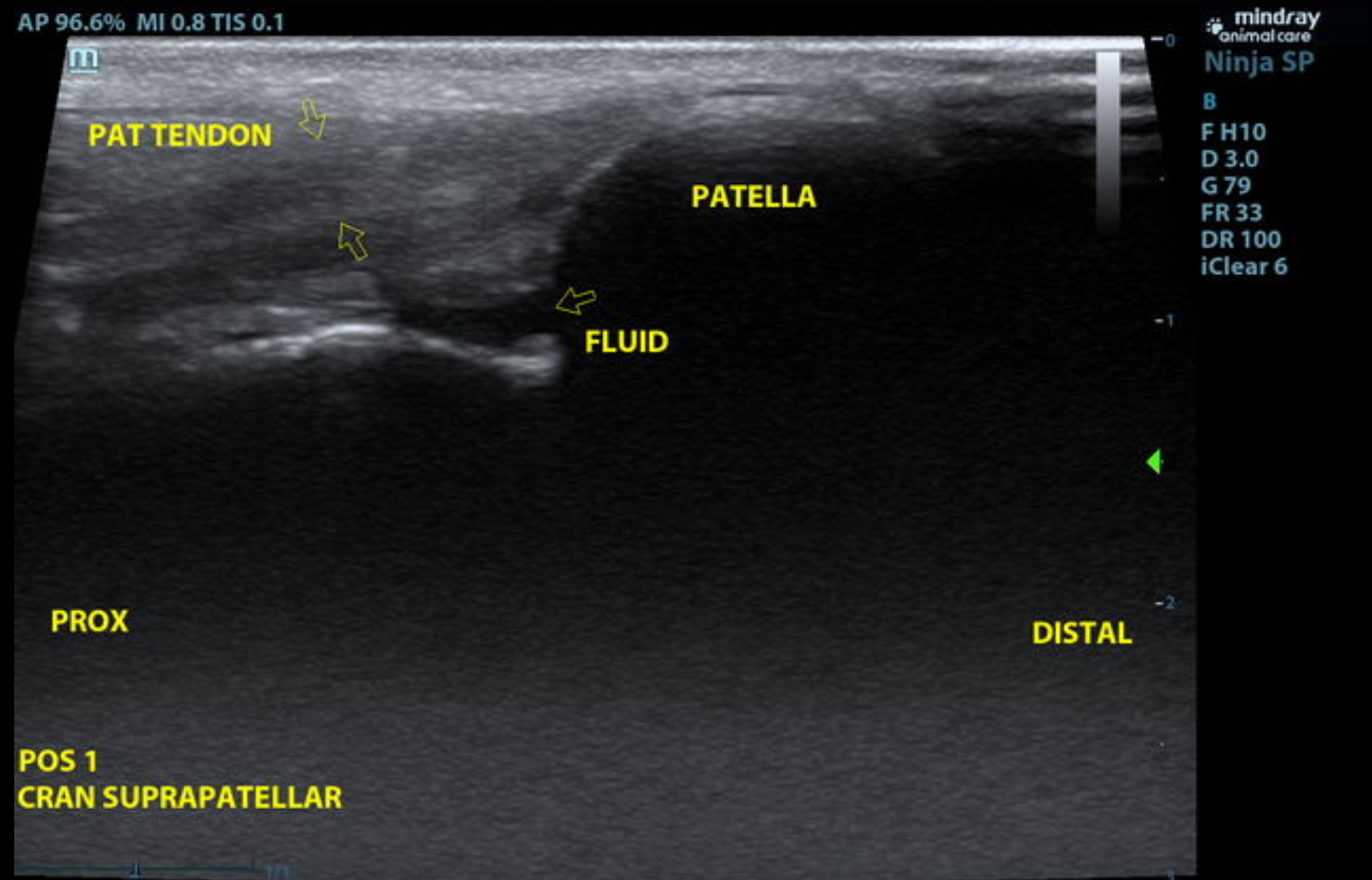
US Video at the cranial suprapatellar position showing fluid ventral to patellar tendon.
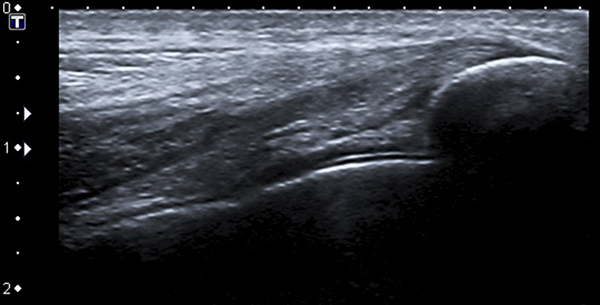
On the left, US image showing a *NORMAL*CCL at Position 2A flexed.
On the right,
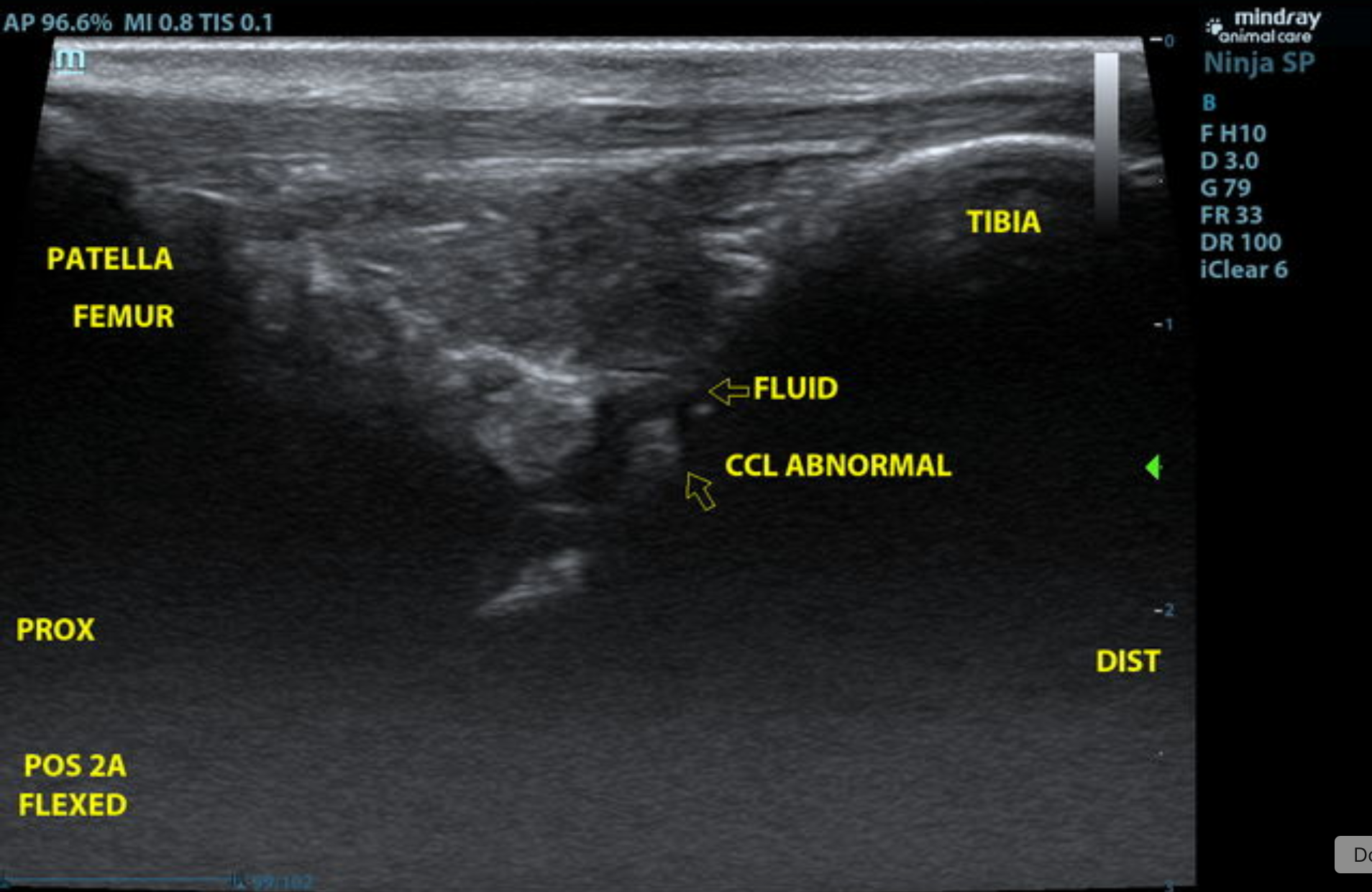
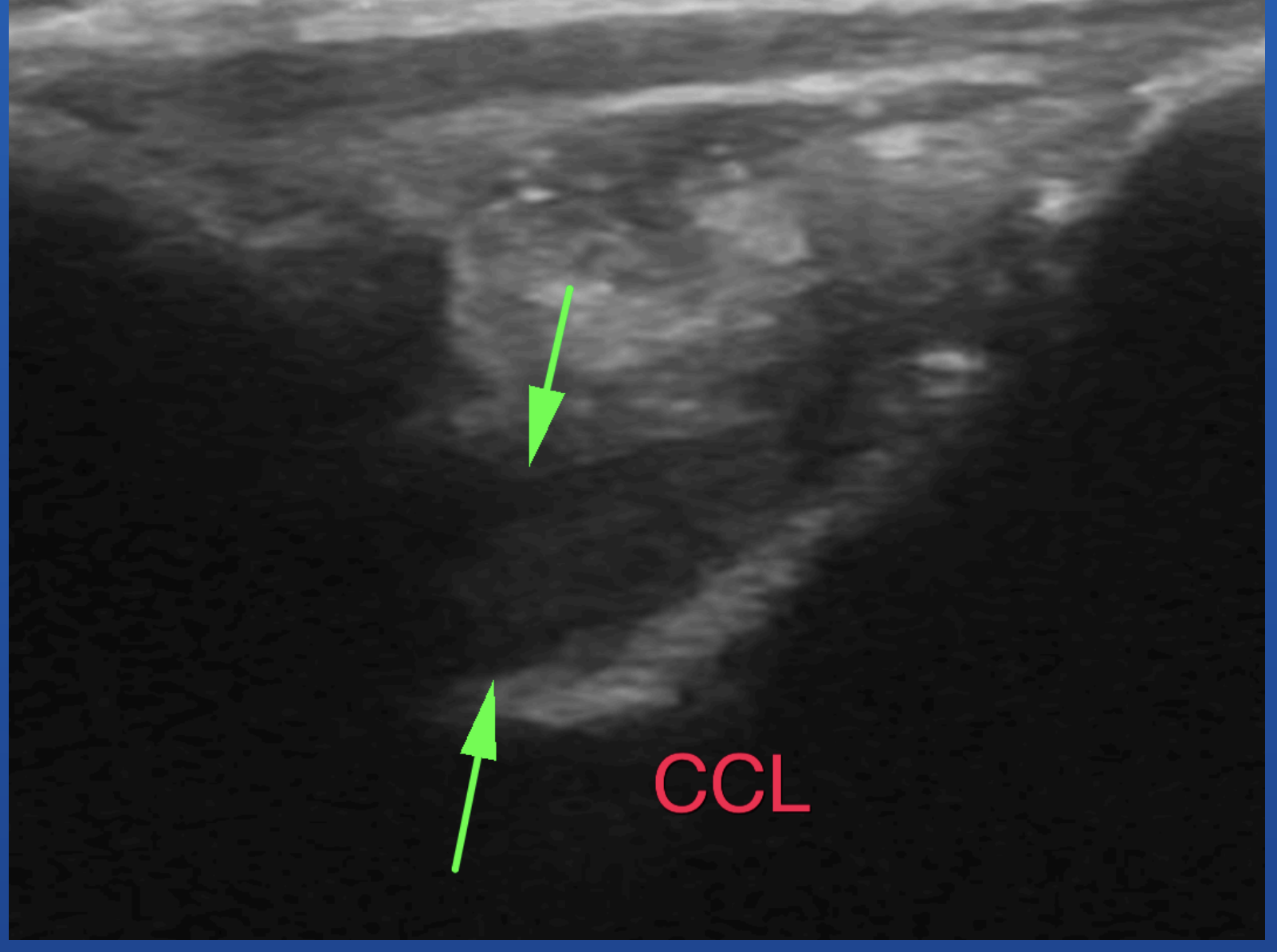
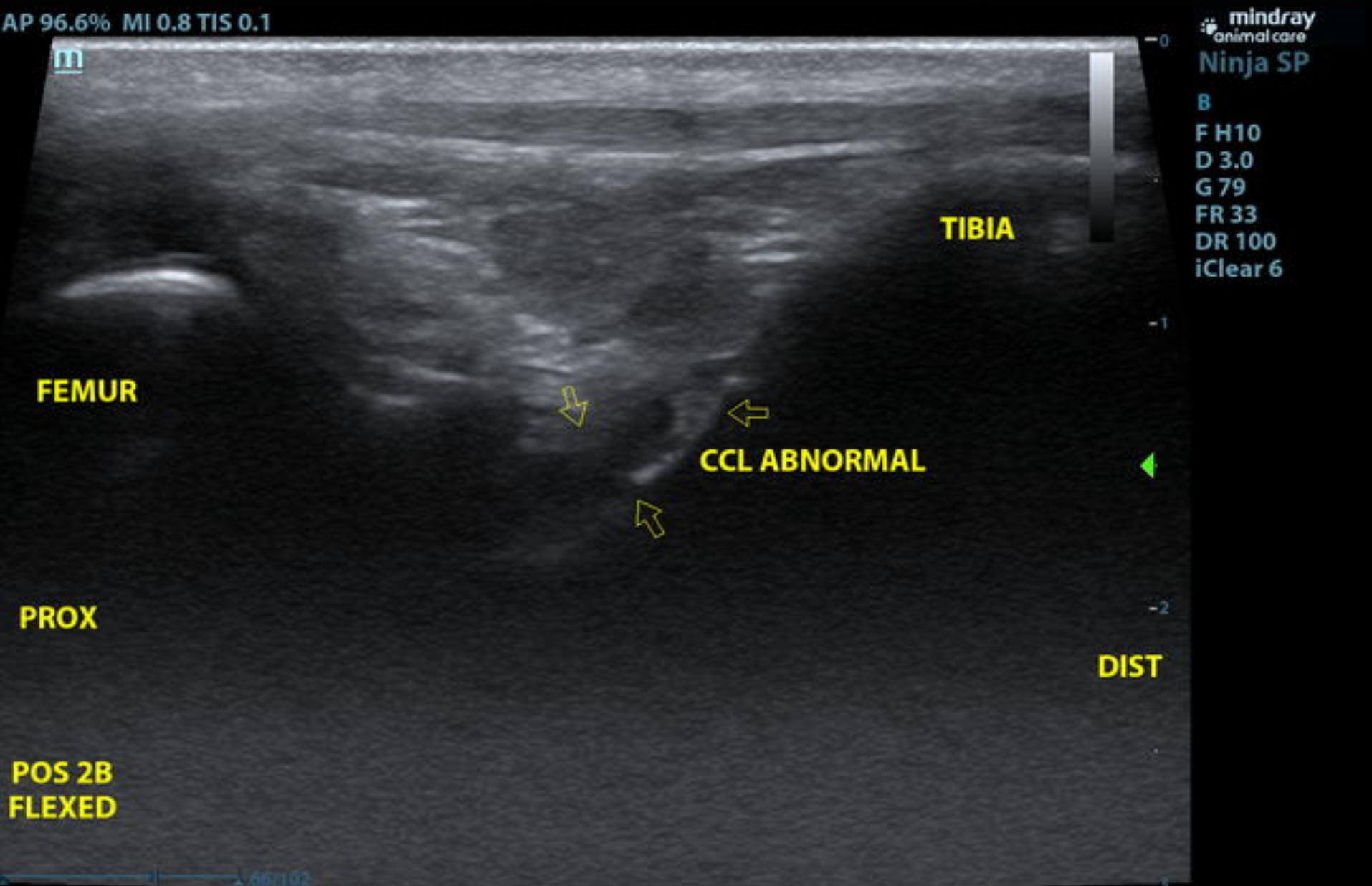
IMAGE: US image at a rotated infrapatellar position with the joint flexed. The abnormal CCL fibers/stump is visible and fluid is present.
VIDEO: US video at a rotated infrapatellar position with the joint flexed. The abnormal CCL fibers/stump is visible with fluid surrounding the ligament.
Left Stifle
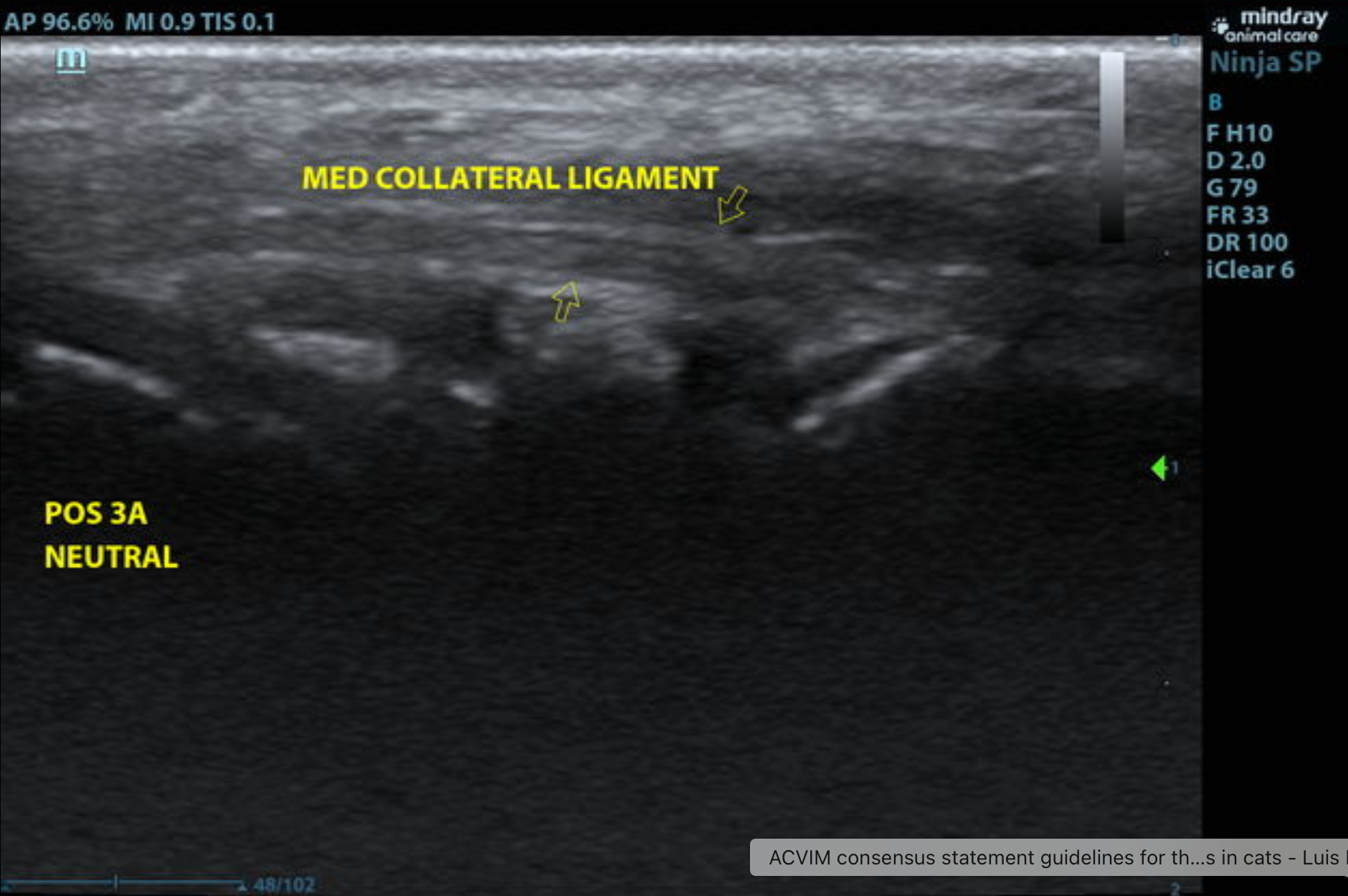
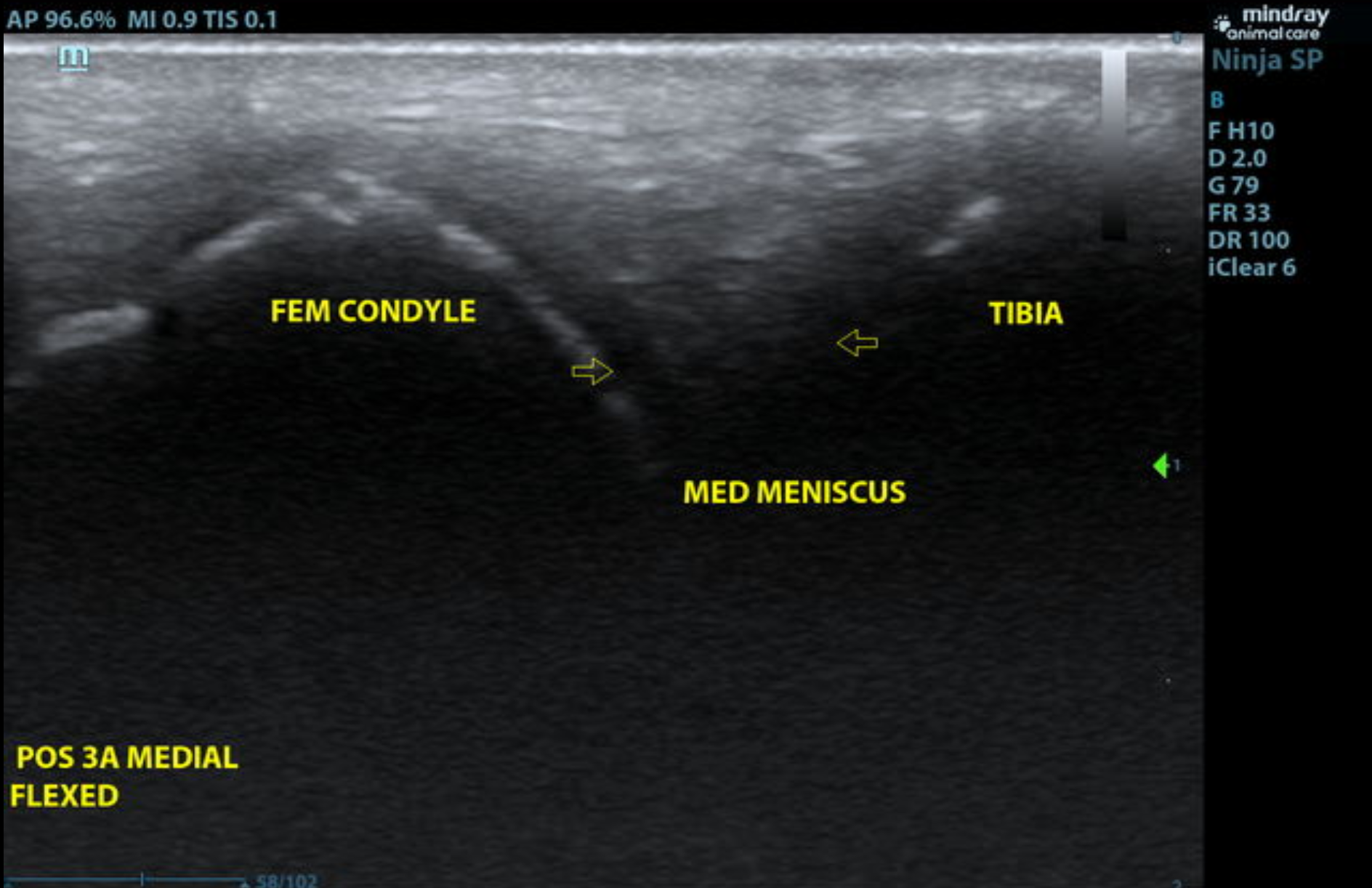
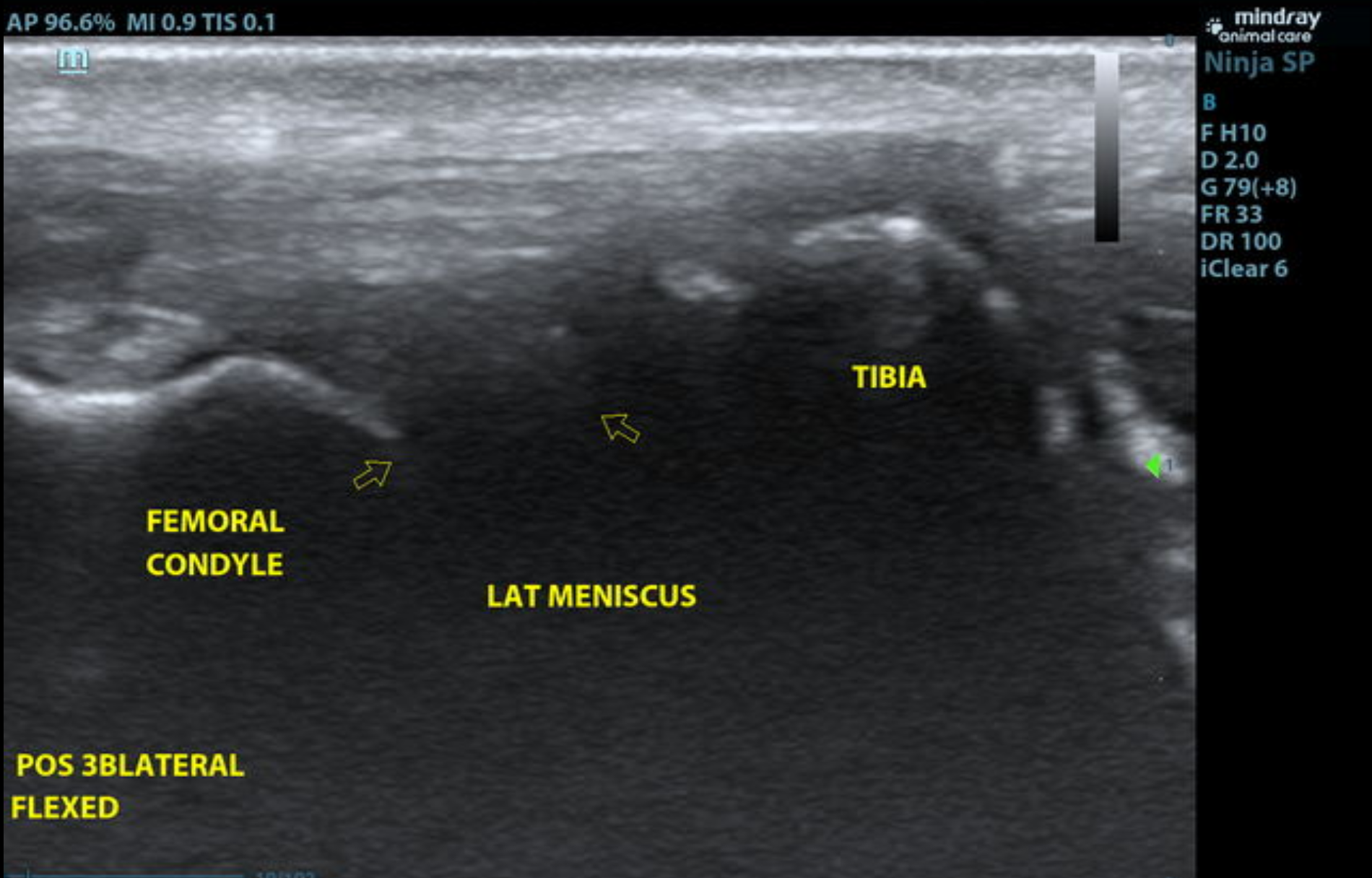
Moderate anechoic effusion and synovial proliferation are noted in the supra- and infra-patellar recesses of the left stifle joint. The medial collateral ligament presents mild thickening. Significant fiber disruption with anechoic halo consistent with effusion surrounding the ligament is seen at the cranial cruciate ligament. The lateral and medial menisci appear normal in position, morphology, and echogenicity. Mild osteophytosis is noted.
• Moderate left stifle effusion and synovitis
• Early degenerative changes
• Partial-to-near complete rupture of the left cranial cruciate ligament
• Menisci remains intact
The ultrasonographic findings are consistent with cranial cruciate ligament pathology and suggest advanced partial to near-complete rupture of the cranial cruciate ligament. No evidence of concomitant meniscal injury is seen at this time. Mild-to-moderate osteoarthritic changes are present. Orthopedic consultation for surgical treatment such as TPLO, TTA, or other surgeon’s preference is recommended.
Cranial cruciate ligament (CCL) rupture is the most common disease of the canine stifle joint. Patellar luxation is also frequently reported. Physical exam is frequently used to elicit cranial drawer, tibial thrust, and patellar luxation and confirm diagnosis. In cases of a partial CCL tear, cranial drawer and tibial thrust may be absent. Radiographic signs of a CCL tear typically include intra-articular swelling, cranial advancement of the tibia, and osteoarthritic changes.
Ultrasonography is a non-invasive, useful tool for assessing cartilage abnormalities, meniscal tears, muscle, tendon and ligament abnormalities, arthropathies, and neoplasia. In a CCL tear the abnormal edges of the ligament can be seen. Ultrasound is very sensitive for partial CCL tears and can be used in dogs in which the cranial drawer is not apparent. MSK US can usually be performed without sedation. There are limitations to ultrasound in evaluating the canine stifle joint. The small joint space allows a limited window for the joint structures to be visualized. Due to the location of the ligament only approximately 30–60% of the distal ligament can be visualized.
The most common findings on ultrasound were hyperechoic changes to the ligament, disruption of the fibers, and irregular bony margins at the insertion of the CCL on the tibia. 123
The patient was referred to a surgeon. On exam, a partial cranial cruciate rupture (~10%) was present, but there was evidence of degeneration in 25–50% of the remnant CCL. The patellar groove was shallow with a moderate amount of wear to the medial ridge. The patella was stabilized with a trochleoplasty, lateral imbrication, and medialization of the proximal tibial segment of the TPLO. The TPLO was performed uneventfully and the knee and patella palpated stable. The patient recovered well from surgery and anesthesia. The patient was sent home on pain medications and a schedule of activity restriction and then slow increase of activity over the next eight weeks.
The Broad Scope of Ultrasound
2 RACE-approved CE credits ($48.99)
Explore the extent to which ultrasound and ultrasound-guided procedures can be applied to nearly every organ system for a fast, efficient and accurate diagnosis!
Orthopedic ultrasound diagnosis
Areas of focus:
- Adrenal pathology
- Pancreatitis
- Gastrointestinal tract
- Liver pathology and presentations
- Urogenital system
MSK US – Stifle: Protocol & Pathologies
1 RACE-approved CE credit ($199.00)
Join Nele Eley, DVM, Dr. med. vet. DipECVDI (Radiology) for this on-demand lecture to learn sonographic approaches for MSK ultrasound of the stifle region. After this course, you will understand common pathologies that affect the stifle, and how to identify them on ultrasound images.
It’s Official! The Digital Edition of The Curbside Guide could be in your pocket in the next fews minutes.
Your Go-To Rereference for everything after the probe.
References
1. Marino DJ, Loughin CA. Diagnostic Imaging of the Canine Stifle: A Review. Veterinary Surgery 2010;39:284–295.
2. Rafla M, Yang P, Mostafa A. Canine Cranial Cruciate Ligament Disease (CCLD): A Concise Review of the Recent Literature. Animals 2025;15. Available at: https://www.mdpi.com/2076-2615/15/7/1030. Accessed April 4, 2026.
3. Tsoi H, Canapp S, Canapp D. Ultrasonographic detection of cranial cruciate ligament pathology in canine stifles without cranio-caudal instability. Veterinary Evidence 2023;8. Available at: https://veterinaryevidence.org/index.php/ve/article/view/632. Accessed April 4, 2026.